The Australian e-Health Research Centre, CSIRO, 147 Underwood Avenue, Floreat, WA, 6014, Australia.
Save Sight Institute, The Faculty of Medicine and Health, The University of Sydney, Sydney, Australia.
BMC Fam Pract. 2021 Nov 30;22(1):239. doi: 10.1186/s12875-021-01586-7.
Despite recent incentives through Medicare (Australia's universal health insurance scheme) to increase retinal screening rates in primary care, comprehensive diabetic retinopathy (DR) screening has not been reached in Australia. The current study aimed to identify key factors affecting the delivery of diabetic retinopathy (DR) screening in Australian general practices.
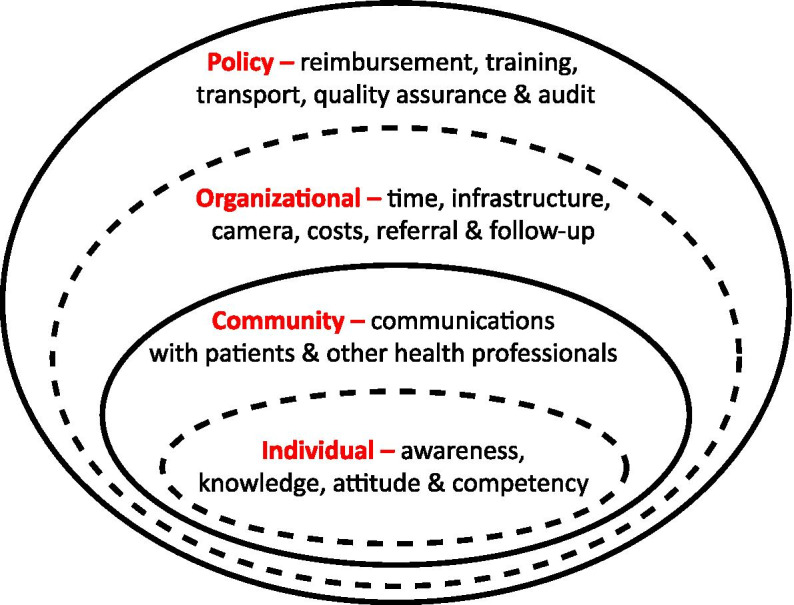
A descriptive qualitative study involving in-depth interviews was carried out from November 2019 to March 2020. Using purposive snowballing sampling, 15 general practitioners (GPs) were recruited from urban and rural general practices in New South Wales and Western Australia. A semi-structured interview guide was used to collect data from participants. All interviews were conducted over the phone by one facilitator, and each interview lasted up to 45 min. The Socio-Ecological Model was used to inform the content of the interview topic guides and subsequent data analysis. Recorded data were transcribed verbatim, and thematic analysis was conducted to identify and classify recurrent themes.
Of 15 GPs interviewed, 13 were male doctors, and the mean age was 54.7 ± 15.5 years. Seven participants were practising in urban areas, while eight were practising in regional or remote areas. All participants had access to a direct ophthalmoscope, but none owned retinal cameras. None of the participants reported performing DR screening. Only three participants were aware of the Medicare Benefits Schedule (MBS) items 12,325 and 12,326 that allow GPs to bill for retinal screening. Seven themes, a combination of facilitators and barriers, emerged from interviews with the GPs. Despite the strong belief in their role in managing chronic diseases, barriers such as costs of retinal cameras, time constraints, lack of skills to make DR diagnosis, and unawareness of Medicare incentives for non-mydriatic retinal photography made it difficult to conduct DR screening in general practice. However, several enabling strategies to deliver DR screening within primary care include increasing GPs' access to continuing professional development, subsidising the cost of retinal cameras, and the need for a champion ace to take the responsibility of retinal photography.
This study identified essential areas at the system level that require addressing to promote the broader implementation of DR screening, in particular, a nationwide awareness campaign to maximise the use of MBS items, improve GPs' competency, and subsidise costs of the retinal cameras for small and rural general practices.
尽管澳大利亚全民医保计划(Medicare)最近出台了激励措施,以提高初级保健中的视网膜筛查率,但澳大利亚仍未全面开展糖尿病视网膜病变(DR)筛查。本研究旨在确定影响澳大利亚全科医生进行糖尿病视网膜病变(DR)筛查的关键因素。
这是一项描述性定性研究,于 2019 年 11 月至 2020 年 3 月期间进行,采用深入访谈法,从新南威尔士州和西澳大利亚州的城市和农村全科医生中招募了 15 名全科医生(GP)。使用有目的的滚雪球抽样法招募参与者,参与者均为男性,年龄在 31 至 70 岁之间,平均年龄为 54.7±15.5 岁。15 名参与者中有 7 名在城市地区执业,8 名在区域或偏远地区执业。所有参与者都可以使用直接检眼镜,但没有一个人拥有视网膜相机。所有参与者均未进行 DR 筛查。只有 3 名参与者了解允许全科医生为视网膜筛查收费的医疗保险福利计划(MBS)项目 12,325 和 12,326。从全科医生的访谈中得出了七个主题,这些主题结合了促进因素和障碍因素。尽管全科医生坚信自己在管理慢性病方面的作用,但由于视网膜相机的成本、时间限制、缺乏 DR 诊断技能以及对非散瞳眼底照相的医疗保险激励措施的认识不足等障碍,使得在全科实践中进行 DR 筛查变得困难。然而,在初级保健中开展 DR 筛查的一些可行策略包括增加全科医生接受继续教育的机会、补贴视网膜相机的成本,以及需要一位有能力的负责人来承担视网膜摄影的责任。
本研究确定了系统层面上需要解决的关键领域,以促进更广泛地开展 DR 筛查,特别是开展全国范围的宣传活动,以最大限度地利用 MBS 项目,提高全科医生的能力,并补贴小型和农村全科医生的视网膜相机成本。