St. Marien-Hospital, Department of Anesthesiology and Intensive Care Medicine, Düren, Germany.
Friedrich-Ebert-Hospital, Department of Anesthesiology and Intensive Care Medicine, Neumünster, Germany.
Braz J Anesthesiol. 2022 Jul-Aug;72(4):484-492. doi: 10.1016/j.bjane.2021.10.007. Epub 2021 Nov 27.
Over 30% of parturients undergoing spinal anesthesia for cesarean section become intraoperatively hypothermic. This study assessed the magnitude of hypothermic insult in parturients and newborns using continuous, high-resolution thermometry and evaluated the efficiency of intraoperative forced-air warming for prevention of hypothermia.
One hundred and eleven parturients admitted for elective or emergency cesarean section under spinal anesthesia with newborn bonding over a 5-month period were included in this retrospective observational cohort study. Patients were divided into two groups: the passive insulation group, who received no active warming, and the active warming group, who received convective warming through an underbody blanket. Core body temperature was continuously monitored by zero-heat-flux thermometry and automatically recorded by data-loggers. The primary outcome was the incidence of hypothermia in the operating and recovery room. Neonatal outcomes were also analyzed.
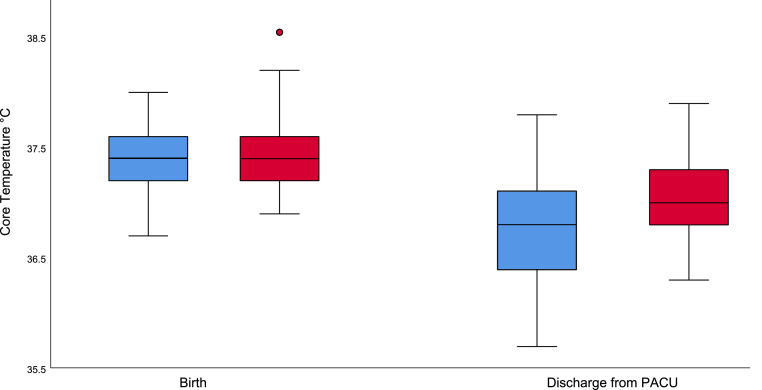
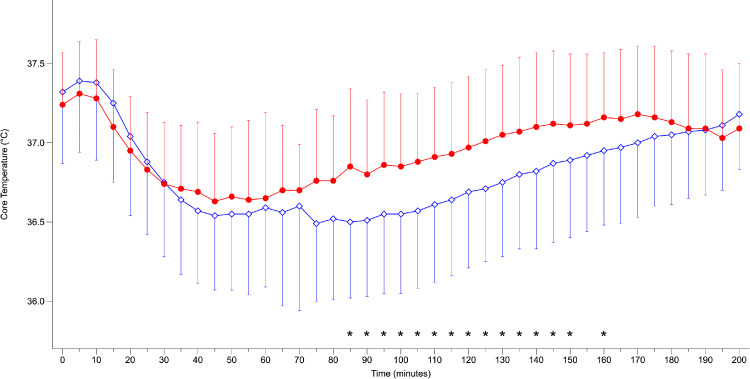
The patients in the passive insulation group had significantly lower temperatures in the operating room compared to the actively warmed group (36.4°C vs. 36.6°C, p = 0.005), including temperature at skin closure (36.5°C vs. 36.7°C, p = 0.017). The temperature of the newborns after discharge from the postanesthetic care unit was lower in the passive insulation group (36.7°C vs. 37.0°C, p = 0.002); thirteen (15%) of the newborns were hypothermic, compared to three (4%) in the active warming group (p < 0.01).
Forced-air warming decreases perioperative hypothermia in parturients undergoing cesarean section but does not entirely prevent hypothermia in newborns while bonding. Therefore, it can be effectively used for cesarean section, but special attention should be given to neonates.
超过 30%行椎管内麻醉行剖宫产术的产妇术中会出现体温过低。本研究通过连续、高分辨率测温法评估产妇和新生儿的低体温损伤程度,并评估术中强制空气加热预防低体温的效果。
本回顾性观察性队列研究纳入了 111 例行椎管内麻醉下择期或紧急剖宫产术并与新生儿进行皮肤接触的产妇,研究时间为 5 个月。患者分为两组:被动保温组,不接受主动加热;主动加热组,通过下体毯子进行对流加热。核心体温通过零热通量测温法连续监测,并由数据记录器自动记录。主要结局是手术和恢复室的低体温发生率。还分析了新生儿结局。
与主动加温组相比,被动保温组患者在手术室的温度明显更低(36.4°C 比 36.6°C,p=0.005),包括皮肤缝合时的温度(36.5°C 比 36.7°C,p=0.017)。离开麻醉后监护室后,被动保温组新生儿的体温较低(36.7°C 比 37.0°C,p=0.002);13 名(15%)新生儿体温过低,而主动加温组仅 3 名(4%)(p<0.01)。
强制空气加热可减少剖宫产术产妇围手术期低体温,但不能完全预防新生儿在皮肤接触时发生低体温。因此,它可有效地用于剖宫产,但应特别注意新生儿。