Institute for Maternal and Child Health IRCCS "Burlo Garofolo", Trieste, Italy.
University of Trieste, Trieste, Italy.
Front Endocrinol (Lausanne). 2021 Nov 9;12:766314. doi: 10.3389/fendo.2021.766314. eCollection 2021.
The purpose of this study was to assess the effectiveness of advanced- (a-HCL) standard-hybrid closed-loop (s-HCL) systems use up to 6 months of treatment in a real-world setting of children and adolescents with T1DM.
We retrospectively evaluated all T1DM pediatric users of MiniMed™ 670G system (s-HCL) and 780G system (a-HCL). HbA1c and BMI were collected at baseline and three and six months after HCL start. Data on glycemic control were extracted from reports generated with CareLink™ Personal Software in Manual Mode, at HCL start, after one, three, and six months after HCL beginning.
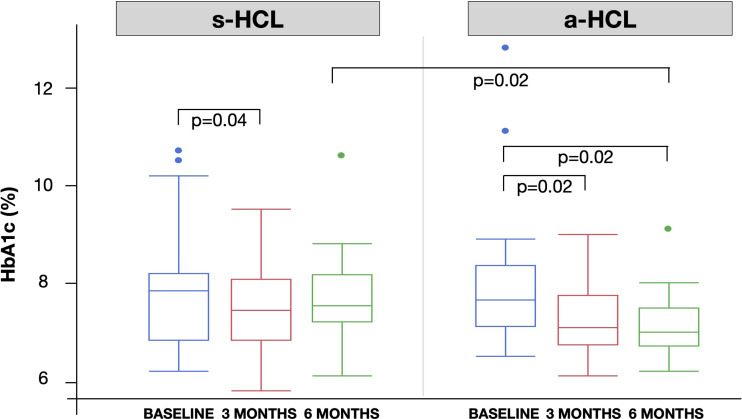
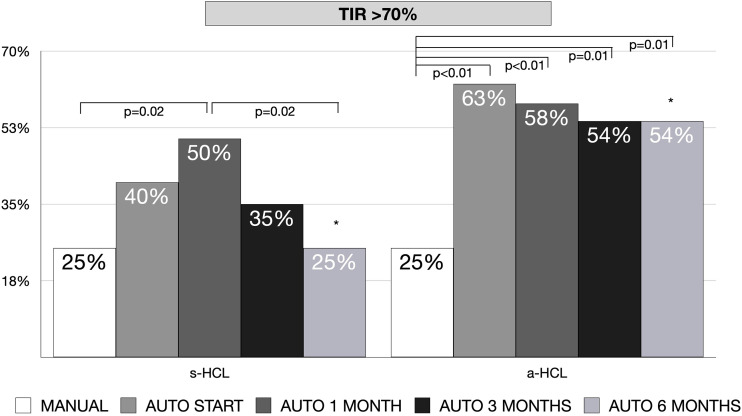
The study included 44 individuals with a median age of 13.3 years (range 2- 21 years), 20 on s-HCL, and 24 on a-HCL. a-HCL users had a significantly lower HbA1c compared to s-HCL after six months of HCL use (7.1 7.7%). Significant differences in HbA1c between a-HCL and s-HCL users were found in children aged 7-14 years (7.1 7.7% after six months) and in those with a worse (HbA1c >8%) glycemic control at the beginning (7.1 8.1% after six months). No significant changes in HbA1c were found in a-HCL users that previously used a s-HCL system. Nevertheless, only the use of a-HCL significantly predicted a lower HbA1c after six months. All sensor-specific measures of glycemic control improved from Manual to Auto mode, in both s-HCL and a-HCL, without increasing time spent in hypoglycemia. However, the percentage of individuals with TIR>70% increased significantly in a-HCL users, who attained this target earlier and more stably: younger age, a higher rate of auto-correction, and a lower amount of CHO inserted predicted a TIR>70%. BMI SDS did not significantly change throughout the study period.
This real-world study suggests that effectiveness might be greater in a-HCL than in s-HCL, with significant changes in HbA1c, and reaching earlier and more stably the target of TIR >70%, without increasing hypoglycemia or BMI. At the same time, previous users of s-HCL systems did not show any further improvement with a-HCL. Children under the age of 14 years of age, not represented in previous studies, seem to benefit the most from a-HCL pumps as well as individuals with the worst glycemic control.
本研究旨在评估高级混合闭环(a-HCL)标准混合闭环(s-HCL)系统在儿童和青少年 1 型糖尿病患者中使用长达 6 个月的治疗效果。
我们回顾性评估了所有使用 MiniMed™ 670G 系统(s-HCL)和 780G 系统(a-HCL)的 T1DM 儿科患者。在 HCL 开始时、3 个月和 6 个月时收集 HbA1c 和 BMI。使用 CareLink™ Personal Software 在 Manual 模式下生成的报告中提取血糖控制数据,在 HCL 开始时、1 个月、3 个月和 6 个月后。
本研究纳入了 44 名中位年龄为 13.3 岁(范围 2-21 岁)的个体,其中 20 名使用 s-HCL,24 名使用 a-HCL。a-HCL 使用者在使用 HCL 6 个月后 HbA1c 显著低于 s-HCL(7.1% vs. 7.7%)。在 7-14 岁的儿童(6 个月后为 7.1% vs. 7.7%)和血糖控制较差(HbA1c>8%)的患者中,a-HCL 使用者与 s-HCL 使用者之间的 HbA1c 差异有统计学意义(6 个月后为 7.1% vs. 8.1%)。在之前使用 s-HCL 系统的 a-HCL 使用者中,HbA1c 没有明显变化。然而,只有使用 a-HCL 才能在 6 个月后显著降低 HbA1c。在 s-HCL 和 a-HCL 中,所有传感器特异性血糖控制测量值均从手动模式改善到自动模式,而不会增加低血糖时间。然而,在 a-HCL 使用者中,TIR>70%的个体比例显著增加,他们更早、更稳定地达到这一目标:年龄较小、自动校正率较高、插入的 CHO 量较低,预测 TIR>70%。在整个研究期间,BMI SDS 没有显著变化。
这项真实世界的研究表明,a-HCL 的疗效可能优于 s-HCL,HbA1c 显著改善,更早、更稳定地达到 TIR>70%的目标,而不会增加低血糖或 BMI。同时,之前使用 s-HCL 系统的患者使用 a-HCL 并没有进一步改善。在之前的研究中没有代表性的 14 岁以下儿童似乎最受益于 a-HCL 泵,以及血糖控制最差的患者。