Institute of Translational Medicine, Department of Molecular and Clinical Cancer Medicine, University of Liverpool, 2nd Floor Sherrington Building, Ashton Street, Liverpool, L69 3GE, UK.
Redx Oncology, Alderley Park, Macclesfield, Cheshire, UK.
J Physiol Biochem. 2023 Feb;79(1):223-234. doi: 10.1007/s13105-021-00857-2. Epub 2021 Dec 5.
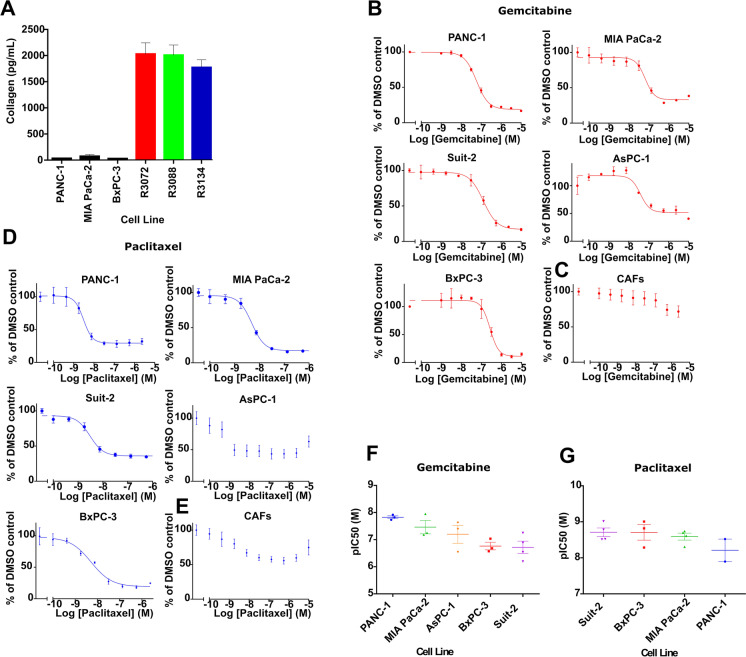
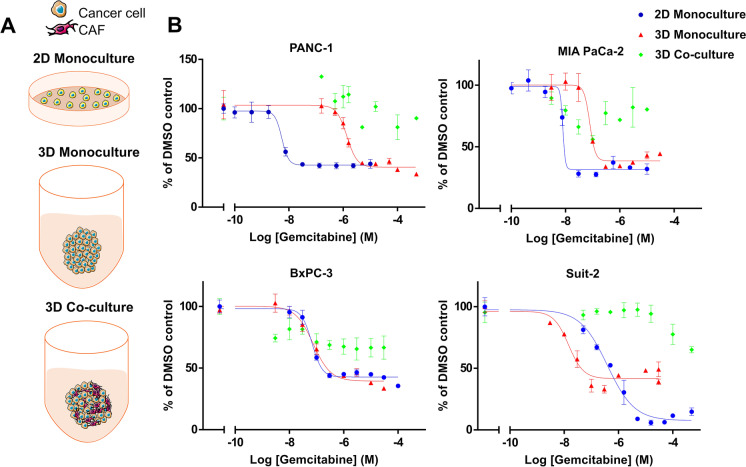
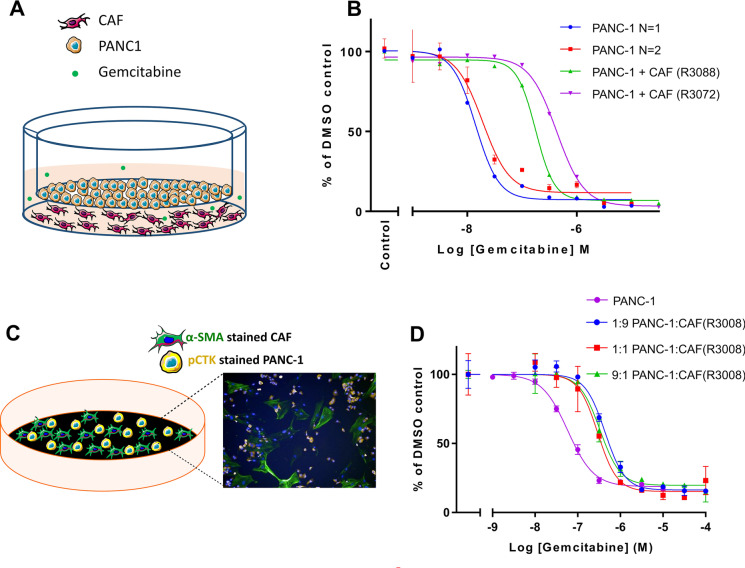
Pancreatic ductal adenocarcinoma (PDAC) is characterised by a pro-inflammatory stroma and multi-faceted microenvironment that promotes and maintains tumorigenesis. However, the models used to test new and emerging therapies for PDAC have not increased in complexity to keep pace with our understanding of the human disease. Promising therapies that pass pre-clinical testing often fail in pancreatic cancer clinical trials. The objective of this study was to investigate whether changes in the drug-dosing regimen or the addition of cancer-associated fibroblasts (CAFs) to current existing models can impact the efficacy of chemotherapy drugs used in the clinic. Here, we reveal that gemcitabine and paclitaxel markedly reduce the viability of pancreatic cell lines, but not CAFs, when cultured in 2D. Following the use of an in vitro drug pulsing experiment, PDAC cell lines showed sensitivity to gemcitabine and paclitaxel. However, CAFs were less sensitive to pulsing with gemcitabine compared to their response to paclitaxel. We also identify that a 3D co-culture model of MIA PaCa-2 or PANC-1 with CAFs showed an increased chemoresistance to gemcitabine when compared to standard 2D mono-cultures a difference to paclitaxel which showed no measurable difference between the 2D and 3D models, suggesting a complex interaction between the drug in study and the cell type used. Changes to standard 2D mono-culture-based assays and implementation of 3D co-culture assays lend complexity to established models and could provide tools for identifying therapies that will match clinically the success observed with in vitro models, thereby aiding in the discovery of novel therapies.
胰腺导管腺癌 (PDAC) 的特征是存在促炎基质和多方面的微环境,促进和维持肿瘤发生。然而,用于测试 PDAC 新出现疗法的模型并没有随着我们对人类疾病的理解而变得更加复杂。在临床试验中,通过临床前测试的有前途的疗法往往会失败。本研究的目的是研究改变药物剂量方案或向当前现有模型中添加癌症相关成纤维细胞 (CAFs) 是否会影响临床上使用的化疗药物的疗效。在这里,我们发现吉西他滨和紫杉醇在 2D 培养时可显著降低胰腺细胞系的活力,但不会降低 CAFs 的活力。在用体外药物脉冲实验后,PDAC 细胞系对吉西他滨和紫杉醇表现出敏感性。然而,与对紫杉醇的反应相比,CAFs 对吉西他滨脉冲的敏感性较低。我们还发现,MIA PaCa-2 或 PANC-1 与 CAFs 的 3D 共培养模型对吉西他滨的化疗耐药性增加,而与紫杉醇相比,2D 和 3D 模型之间没有可测量的差异,这表明研究中的药物与所用细胞类型之间存在复杂的相互作用。对标准 2D 单培养为基础的测定方法的改变和 3D 共培养测定方法的实施为已建立的模型增加了复杂性,并可为鉴定与体外模型观察到的临床成功相匹配的疗法提供工具,从而有助于发现新的疗法。