Department of Liver Surgery & Liver Transplantation, State Key Laboratory of Biotherapy and Cancer Center, West China Hospital, Sichuan University and Collaborative Innovation Center of Biotherapy, Chengdu, China.
Cancer Med. 2022 Jan;11(2):317-331. doi: 10.1002/cam4.4448. Epub 2021 Dec 5.
The prognostic value of sarcopenia in combined hepatocellular carcinoma and cholangiocarcinoma (cHCC-CC) patients after surgery has not been evaluated, while the efficacy of the available tumor stage for cHCC-CC remains controversial.
All consecutive cHCC-CC patients after surgery were retrieved. The patients were stratified by the sex-specific medians of the psoas muscle index into groups with or without sarcopenia. Prognosis was analyzed using the Kaplan-Meier (K-M) method, and the K-M curves were adjusted by inverse probability weighting (IPW). A nomogram based on Cox regression analysis was established and further compared with primary liver cancer (PLC) stages by internal validation based on bootstrap resampling and k-fold cross-validation.
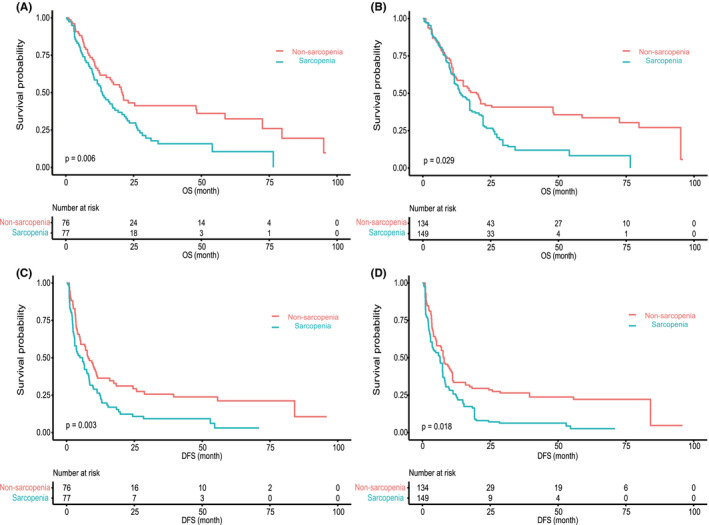
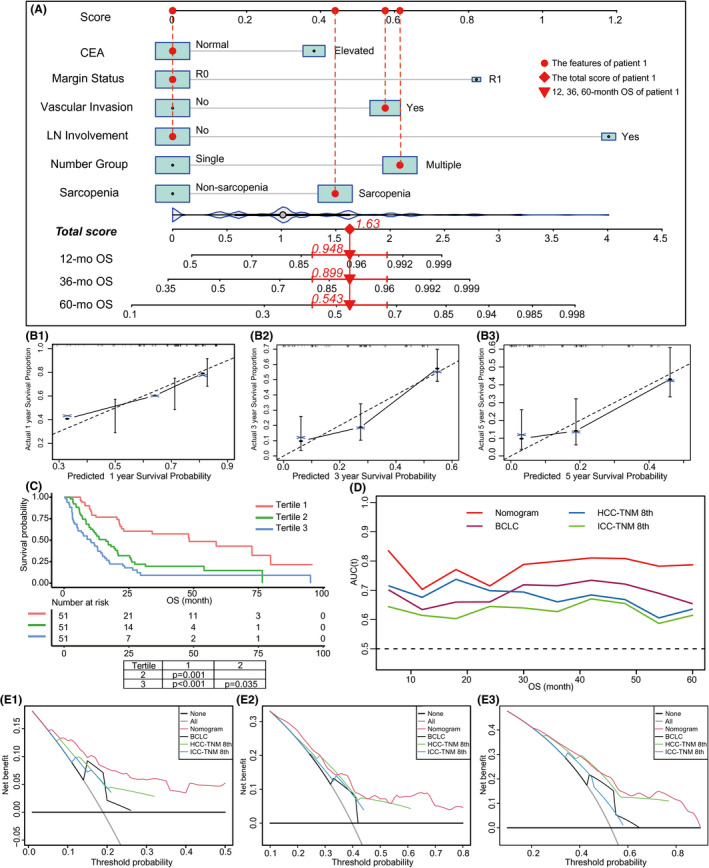
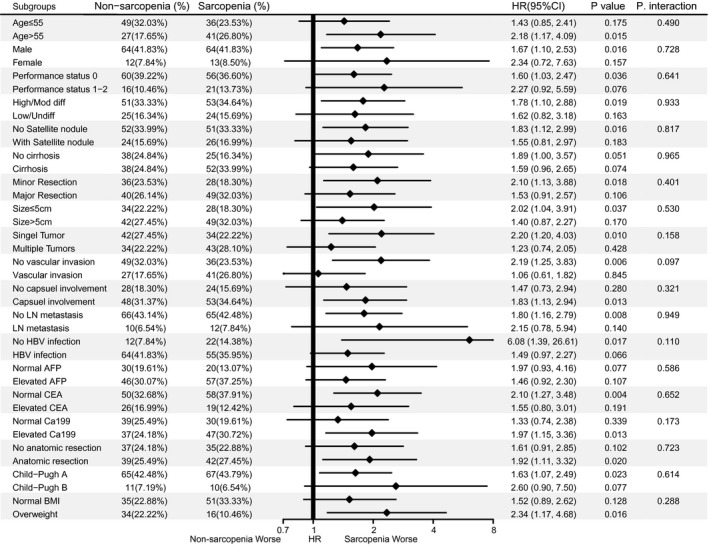
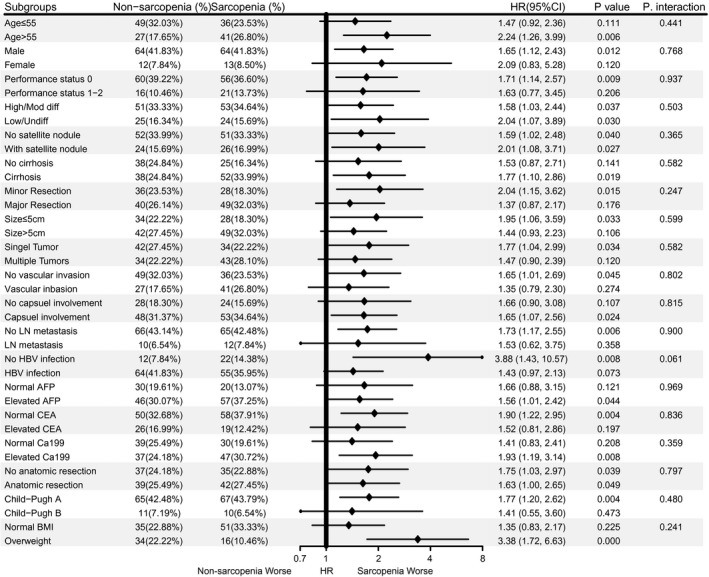
A total of 153 patients were stratified into sarcopenia and non-sarcopenia groups. The sarcopenia group revealed statistically worse overall survival (OS) and disease-free survival (DFS) using the K-M method and K-M curves adjusted by IPW. Multivariate Cox regression analyses suggested sarcopenia as an independent risk factor for OS (HR = 1.55; p = 0.040) and DFS (HR = 1.55; p = 0.019). Subgroup analysis based on baseline variables showed sarcopenia as a stable risk factor for the prognosis. Our nomogram outperformed PLC stages in prognostic prediction, as evidenced by the best c-index, area under the curve, and positive improvement of the net reclassification index and integrated discrimination improvement. A fivefold cross-validation revealed consistent results. Decision curve analysis revealed higher net benefits of the nomogram than PLC stages.
Sarcopenia is an independent and stable risk factor for the prognosis of cHCC-CC patients after surgery. Our nomogram might aid high-risk patient identification and clinical decisions.
目前尚未评估肌少症对接受手术治疗后的肝细胞癌合并胆管细胞癌(cHCC-CC)患者的预后价值,而现有的肿瘤分期对 cHCC-CC 的疗效仍存在争议。
本研究回顾性分析了所有接受手术治疗后的 cHCC-CC 患者。根据竖脊肌指数的性别特异性中位数,将患者分为肌少症组和非肌少症组。采用 Kaplan-Meier(K-M)法分析预后,并采用逆概率加权(IPW)调整 K-M 曲线。基于 Cox 回归分析建立列线图,并通过内部验证(基于 bootstrap 重采样和 k 折交叉验证)与原发性肝癌(PLC)分期进行比较。
共 153 例患者被分为肌少症组和非肌少症组。K-M 法和 IPW 调整后的 K-M 曲线显示,肌少症组的总生存(OS)和无病生存(DFS)均较差。多因素 Cox 回归分析表明,肌少症是 OS(HR=1.55;p=0.040)和 DFS(HR=1.55;p=0.019)的独立危险因素。基于基线变量的亚组分析表明,肌少症是预后的稳定危险因素。我们的列线图在预后预测方面优于 PLC 分期,表现为最佳 C 指数、曲线下面积以及净重新分类指数和综合判别改善的阳性改善。五重交叉验证结果一致。决策曲线分析表明,列线图的净获益高于 PLC 分期。
肌少症是 cHCC-CC 患者手术后预后的独立且稳定的危险因素。我们的列线图可能有助于高危患者的识别和临床决策。