Department of Pediatrics, Diabetology, Endocrinology and Nephrology, Medical University of Lodz, Lodz, Poland.
Department of Medical Immunology, Medical University of Gdansk, Gdansk, Poland.
Front Immunol. 2021 Nov 17;12:742834. doi: 10.3389/fimmu.2021.742834. eCollection 2021.
Autoimmune disorders, IgA deficiency, and allergies seem to be common among individuals with 18q deletion syndrome [OMIM 601808]. We aimed to determine the prevalence, mechanism, and genetic background of autoimmunity, immune deficiency, and allergy in a cohort of patients with 18q deletions.
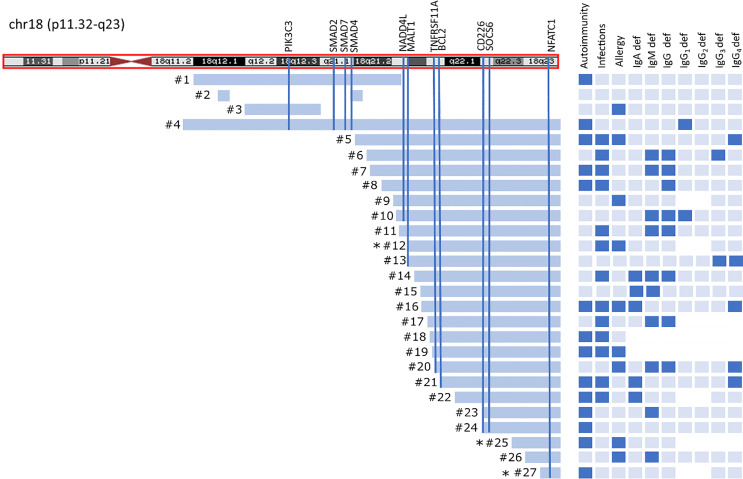
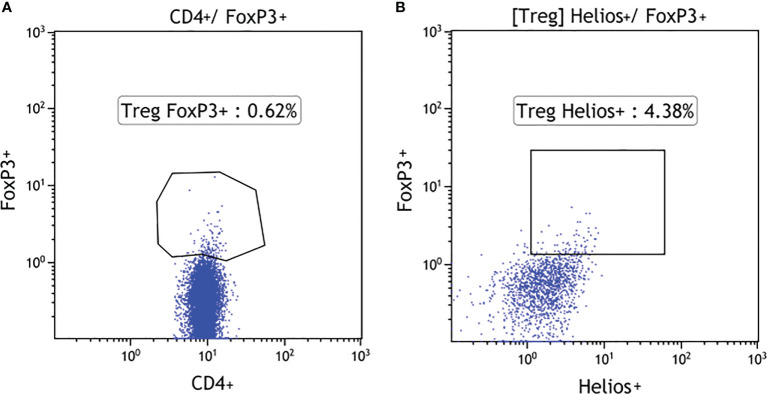
Medical registries and social media were used to recruit the patients. Microarray oligonucleotide comparative genomic hybridization (aCGH) (Agilent, Santa Clara, CA, USA) was performed in all patients to identify size and location of chromosome 18 deletion. Clinical evaluation and medical record collection were performed in each of the study participants. The history of autoimmune disorders, severe and/or recurrent infections, and symptoms of allergy were noted. Total immunoglobulin IgG, IgA, IgM, IgE, and IgG serum levels were measured using nephelometry and ELISA methods. Lymphocyte T subset phenotyping was performed in 24 subjects from 18q del cohort. To predict the most promising candidate genes, we used the ENDEAVOUR-a free web resource for gene prioritization.
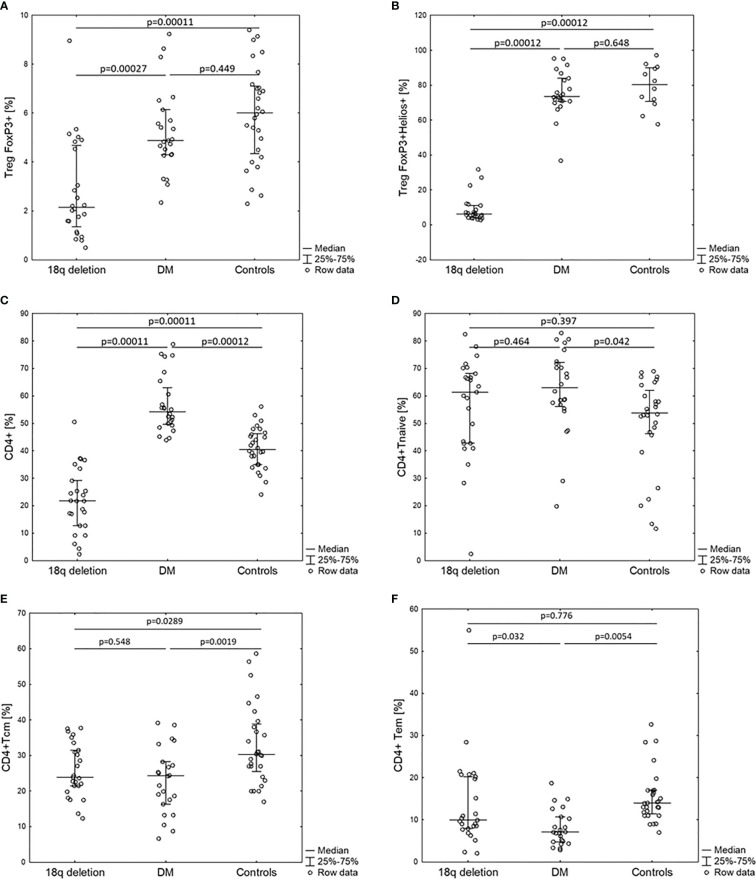
18q deletion was confirmed by means of array CGH analysis in 27 individuals, 15 (55.6%) females and 12 males, referred to the project by specialists in medical genetics, diabetology, or pediatric endocrinology between May 2015 and December 2019. The mean age at examination was 11.8 years (min-max: 4.0-33.5). Autoimmune disorders were present in 14/27 (51.8%) of the cohort. In eight of patients, symptoms of immune deficiency coexisted with autoimmunity. Allergy was reported in nine of 27 (33.4%) patients. Over 89% of patients presented with at list one type of immunoglobulin (IgA, IgM, IgG, IgE, and IgG) deficiency and eight of 25 (32%) had abnormalities in at least two major immunoglobulin (IgG, IgA, IgM) measurements (CVID-like phenotype). Patients with 18q del exhibited a significantly decreased CD4, Treg FOXP3+, TregFOXP3+Helios+, and TemCD4 cell numbers in comparison with the control groups of 24 T1DM patients and 28 healthy controls.
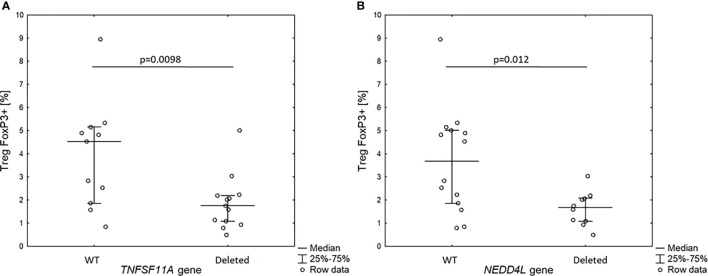
Patients with 18q deletions frequently suffer from autoimmune disorders, recurrent infections, and allergy due to immune dysregulation presenting with variable antibody deficiencies and T-regulatory cell deficiency (CD4+CD25+CD127lowFOXP3+). The spectrum of speculations regarding which gene might be responsible for such phenotype ranges from single gene haploinsufficiency to deletion of a cluster of immunogenes located distally to 18q21.
自身免疫性疾病、IgA 缺乏症和过敏似乎在 18q 缺失综合征患者中很常见[OMIM 601808]。我们旨在确定一组 18q 缺失患者中自身免疫、免疫缺陷和过敏的患病率、机制和遗传背景。
使用医疗登记册和社交媒体招募患者。对所有患者进行微阵列寡核苷酸比较基因组杂交(aCGH)(Agilent,加利福尼亚州圣克拉拉),以确定 18 号染色体缺失的大小和位置。对每位研究参与者进行临床评估和病历收集。记录自身免疫性疾病、严重和/或反复感染以及过敏症状的病史。使用比浊法和 ELISA 方法测量总免疫球蛋白 IgG、IgA、IgM、IgE 和 IgG 血清水平。对 18q 缺失队列中的 24 名受试者进行淋巴细胞 T 亚群表型分析。为了预测最有前途的候选基因,我们使用了 ENDEAVOUR-一个免费的基因优先级网络资源。
通过 2015 年 5 月至 2019 年 12 月,医学遗传学、糖尿病学或儿科内分泌学专家推荐,通过微阵列 CGH 分析在 27 名个体中证实了 18q 缺失,其中 15 名(55.6%)为女性,12 名为男性。接受检查的平均年龄为 11.8 岁(最小-最大:4.0-33.5)。27 名队列中的 14 名(51.8%)患有自身免疫性疾病。在 8 名患者中,免疫缺陷的症状与自身免疫同时存在。27 名患者中有 9 名(33.3%)报告有过敏。超过 89%的患者至少有一种免疫球蛋白(IgA、IgM、IgG、IgE 和 IgG)缺乏,25 名患者中有 8 名(32%)至少有两种主要免疫球蛋白(IgG、IgA、IgM)测量值异常(CVID 样表型)。与 24 名 T1DM 患者和 28 名健康对照组相比,18q del 患者的 CD4、Treg FOXP3+、TregFOXP3+Helios+和 TemCD4 细胞数量显著减少。
由于免疫失调导致抗体和 T 调节细胞(CD4+CD25+CD127lowFOXP3+)的数量出现可变的缺乏,患有 18q 缺失的患者经常患有自身免疫性疾病、反复感染和过敏。关于哪些基因可能导致这种表型的推测范围从单个基因单倍不足到 18q21 远端免疫基因簇的缺失。