Chen Xinyu, Lai Lin, Ye Jiazhou, Li Lequn
Department of Hepatobiliary Surgery, Guangxi Medical University Cancer Hospital, Nanning, China.
Department of Medical Oncology, The First Affiliated Hospital of Guangxi Medical University, Nanning, China.
Front Oncol. 2021 Nov 19;11:740762. doi: 10.3389/fonc.2021.740762. eCollection 2021.
Hepatocellular carcinoma (HCC) is a high-grade malignant disease with unfavorable prognosis, and although surgical therapy is necessary, not all patients with HCC are suitable candidates for surgery. Downstaging as preoperative therapeutic strategy, which can convert unresectable HCC into resectable HCC, intends to increase the resection rate and improve prognosis.
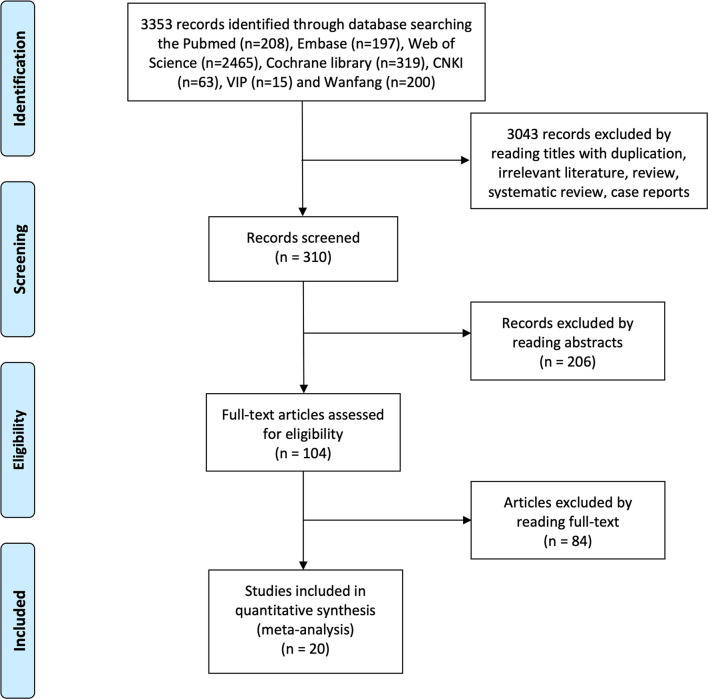
We searched multiple databases updated to December 30, 2020, for studies on transcatheter arterial chemoembolization (TACE), Yttrium 90 microsphere selective internal radiation (SIR)/transcatheter radioembolization (TARE), hepatic arterial infusion (HAI), and systemic treatment as downstaging treatment before resection for patients with unresectable HCC.
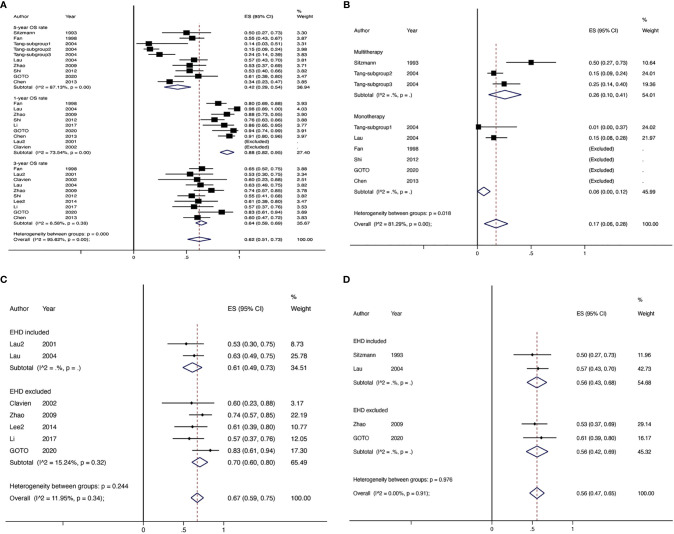
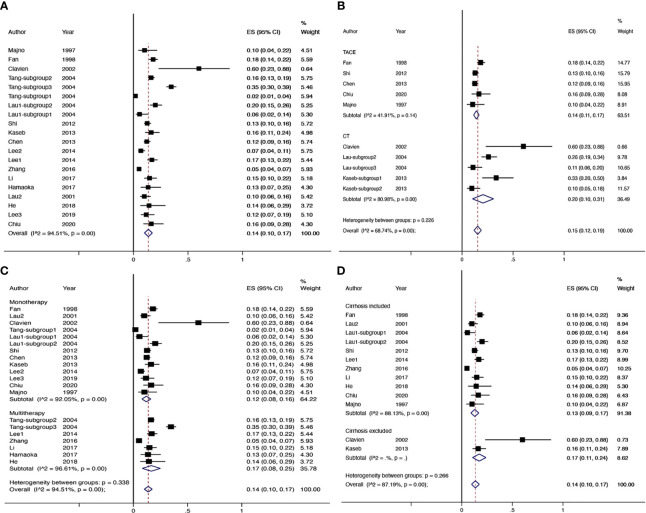
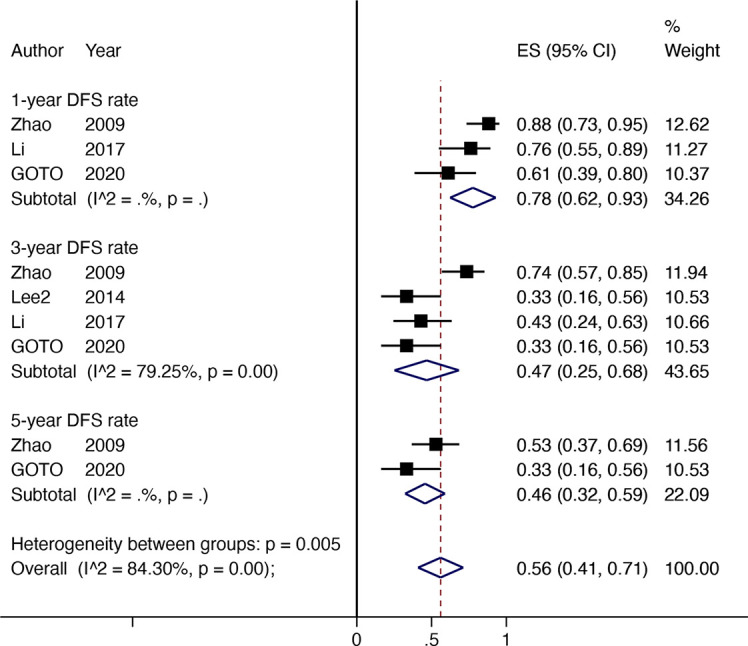
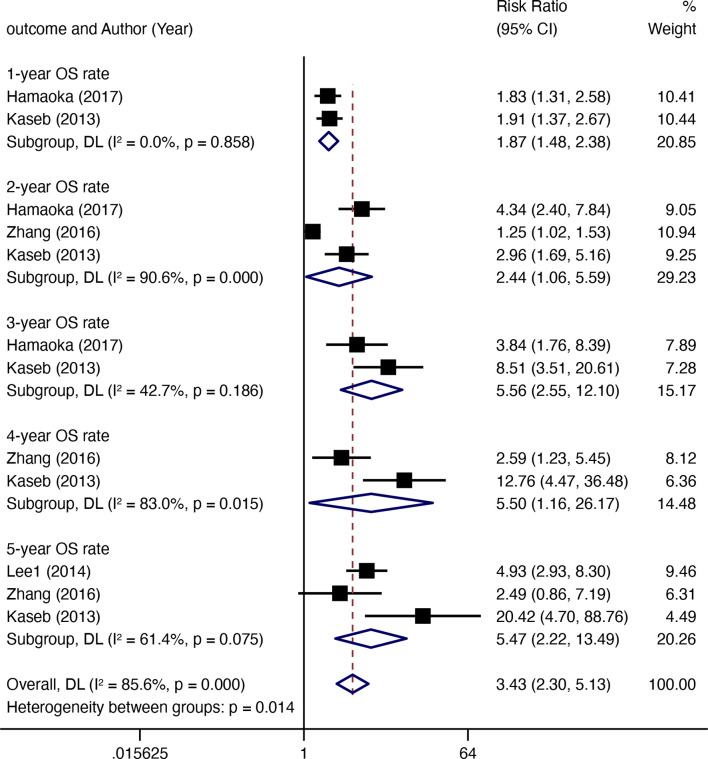
A total of 20 comparative and non-comparative studies were finally included in the meta-analysis. The pooled downstaging rate of hepatic resection (HR) was 14% [95% confidence interval (CI) 0.10-0.17] with significant heterogeneity ( = 94.51%). The chemotherapy, combination, and non-cirrhosis groups exhibit higher rates of downstaging, but these differences were not significant. For comparative studies, the overall survival (OS) rates of resection after downstaging were far better than those inpatients who received locoregional therapy (LRT) or systemic treatment alone at 1 year (RR 1.87, 95% CI 1.48-2.38), 3 years (RR 5.56, 95% CI 2.55-12.10), and 5 years (RR 5.47, 95% CI 2.22-13.49). In addition, the pooled disease-free survival (DFS) rates in patients undergoing HR after successful downstaging were 78% (95% CI 0.62-0.93) at 1 year, 47% (95% CI 0.25-0.68) at 3 years, and 46% (95% CI 0.32-0.59) at 5 years. The pooled OS rates were 88% (95% CI 0.82-0.95) at 1 year, 64% (95% CI 0.59-0.69) at 3 years, and 42% (95% CI 0.29-0.54) at 5 years.
Downstaging may serve as a screening tool to identify patients who might benefit from surgery. Resection after successful downstaging can improve prognosis.
肝细胞癌(HCC)是一种预后不良的高度恶性疾病,虽然手术治疗是必要的,但并非所有HCC患者都适合手术。术前进行降期治疗作为一种治疗策略,可将不可切除的HCC转化为可切除的HCC,旨在提高切除率并改善预后。
我们检索了截至2020年12月30日更新的多个数据库,以查找关于经动脉化疗栓塞术(TACE)、钇90微球选择性内照射(SIR)/经动脉放射性栓塞术(TARE)、肝动脉灌注(HAI)以及全身治疗作为不可切除HCC患者术前降期治疗的研究。
共有20项比较性和非比较性研究最终纳入荟萃分析。肝切除(HR)的汇总降期率为14%[95%置信区间(CI)0.10 - 0.17],具有显著异质性(I² = 94.51%)。化疗组、联合治疗组和非肝硬化组的降期率较高,但这些差异不显著。对于比较性研究,降期后切除的1年总体生存率(OS)远优于仅接受局部区域治疗(LRT)或全身治疗的患者(RR 1.87,95% CI 1.48 - 2.38)、3年(RR 5.56,95% CI 2.55 - 12.10)和5年(RR 5.47,95% CI 2.22 - 13.49)。此外,成功降期后接受HR患者的1年汇总无病生存率(DFS)为78%(95% CI 0.62 - 0.93)、3年为47%(95% CI 0.25 - 0.68)、5年为46%(95% CI 0.32 - 0.59)。汇总OS率1年为88%(95% CI 0.82 - 0.95)、3年为64%(95% CI 0.59 - 0.69)、5年为42%(95% CI 0.29 - 0.54)。
降期可作为一种筛选工具,用于识别可能从手术中获益的患者。成功降期后进行切除可改善预后。