Bagnasco Diego, Paggiaro Pierluigi, Latorre Manuela, Folli Chiara, Testino Elisa, Bassi Arianna, Milanese Manlio, Heffler Enrico, Manfredi Andrea, Riccio Anna Maria, De Ferrari Laura, Blasi Francesco, Canevari Rikki Frank, Canonica Giorgio Walter, Passalacqua Giovanni
Allergy and Respiratory Diseases, Department of Internal Medicine (DIMI), IRCCS Policlinico San Martino, University of Genoa, Italy.
Department of Surgery, Medicine, Molecular Biology and Critical Care, University of Pisa, Italy.
World Allergy Organ J. 2021 Nov 19;14(11):100606. doi: 10.1016/j.waojou.2021.100606. eCollection 2021 Nov.
There is, so far, no universal definition of severe asthma. This definition usually relies on: number of exacerbations, inhaled therapy, need for oral corticosteroids, and respiratory function. The use of such parameters varies in the different definitions used. Thus, according to the parameters chosen, each patient may result in having severe asthma or not. The aim of this study was to evaluate how the choice of a specific definition of severe asthma can change the allocation of patients.
Data collected from the Severe Asthma Network Italy (SANI) registry were analyzed. All the patients included were then reclassified according to the definitions of U-BIOPRED, NICE, WHO, ATS/ERS, GINA, ENFUMOSA, and TENOR.
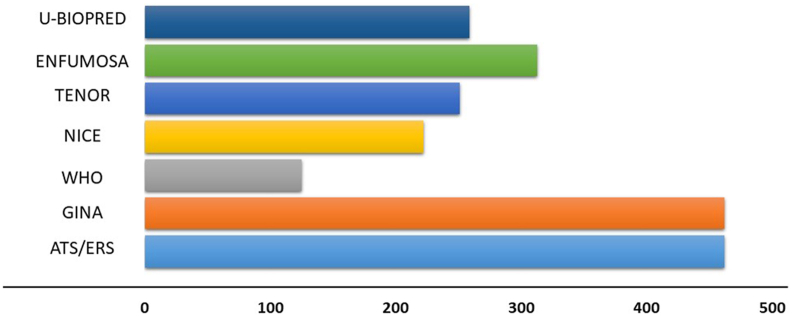
540 patients, were extracted from the SANI database. We observed that 462 (86%) met the ATS/ERS criteria as well as the GINA criteria, 259 (48%) the U-Biopred, 222 (41%) the NICE, 125 (23%) the WHO, 313 (58%) the Enfumosa, and 251 (46%) the TENOR criteria. The mean eosinophil value were similar in the ATS/ERS, U-Biopred, and Enfumosa (528, 532 and 516 cells/mcl), higher in WHO and Tenor (567 and 570 cells/mcl) and much higher in the NICE classification (624 cells/mcl). Lung function tests resulted similarly in all groups, with WHO (67%) and ATS/ERS-GINA (73%), respectively, showing the lower and upper mean FEV1 values.
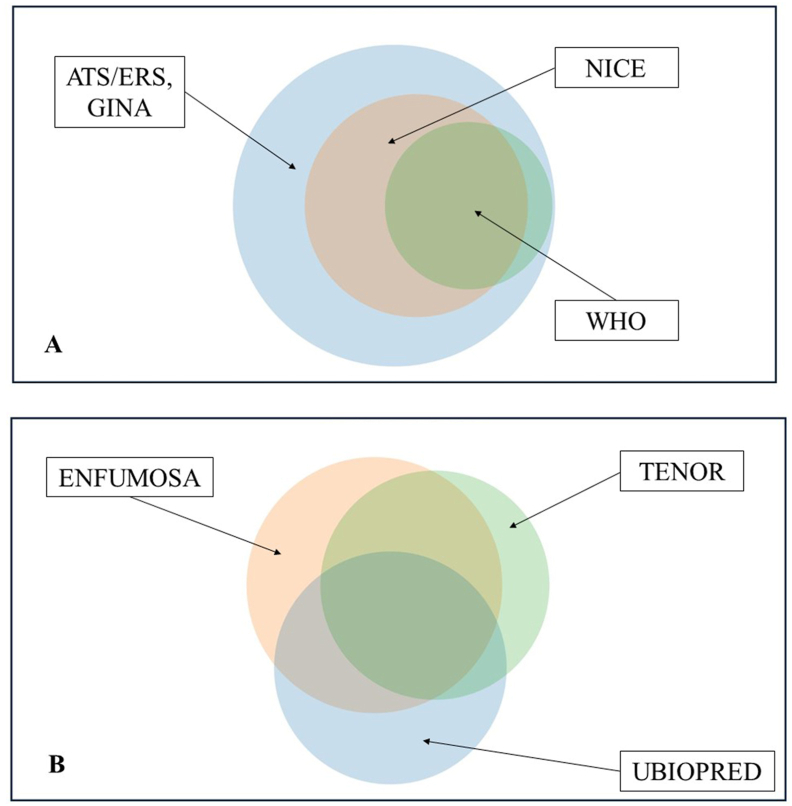
The present observations clearly evidence the heterogeneity in the distribution of patients when different definitions of severe asthma are used. However, the recent definition of severe asthma, provided by the GINA document, is similar to that indicated in 2014 by ATS/ERS, allowing mirror reclassification of the patients examined. This lack of homogeneity could complicate the access to biological therapies. The definition provided by the GINA document, which reflects what suggested by ATS/ERS, could partially overcome the problem.
到目前为止,重度哮喘尚无统一的定义。该定义通常依赖于:发作次数、吸入治疗、口服糖皮质激素的需求以及呼吸功能。在不同的定义中,这些参数的使用各不相同。因此,根据所选择的参数,每个患者可能被判定为患有重度哮喘或未患有重度哮喘。本研究的目的是评估重度哮喘特定定义的选择如何改变患者的分类。
对从意大利重度哮喘网络(SANI)登记处收集的数据进行分析。然后根据U-BIOPRED、英国国家卫生与临床优化研究所(NICE)、世界卫生组织(WHO)、美国胸科学会/欧洲呼吸学会(ATS/ERS)、全球哮喘防治创议(GINA)、欧洲多中心哮喘研究(ENFUMOSA)和欧洲呼吸学会/欧洲变态反应与临床免疫学会(TENOR)的定义,对所有纳入的患者重新进行分类。
从SANI数据库中提取了540例患者。我们观察到,462例(86%)符合ATS/ERS标准以及GINA标准,259例(48%)符合U-BIOPRED标准,222例(41%)符合NICE标准,125例(23%)符合WHO标准,313例(58%)符合ENFUMOSA标准,251例(46%)符合TENOR标准。在ATS/ERS、U-BIOPRED和ENFUMOSA中,嗜酸性粒细胞平均数值相似(分别为每微升528、532和516个细胞),在WHO和TENOR中较高(分别为每微升567和570个细胞),在NICE分类中则高得多(每微升624个细胞)。所有组的肺功能测试结果相似,WHO组(67%)和ATS/ERS-GINA组(73%)分别显示出较低和较高的平均第1秒用力呼气容积(FEV1)值。
目前的观察结果清楚地证明,当使用不同的重度哮喘定义时,患者分布存在异质性。然而,GINA文件提供的重度哮喘最新定义与ATS/ERS在2014年指出的定义相似,使得所检查患者能够进行镜像重新分类。这种缺乏同质性可能会使生物疗法的获取变得复杂。GINA文件提供的定义反映了ATS/ERS的建议,可能会部分克服这一问题。