Br J Surg. 2021 Dec 1;108(12):1448-1464. doi: 10.1093/bjs/znab336.
This study aimed to determine the impact of pulmonary complications on death after surgery both before and during the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic.
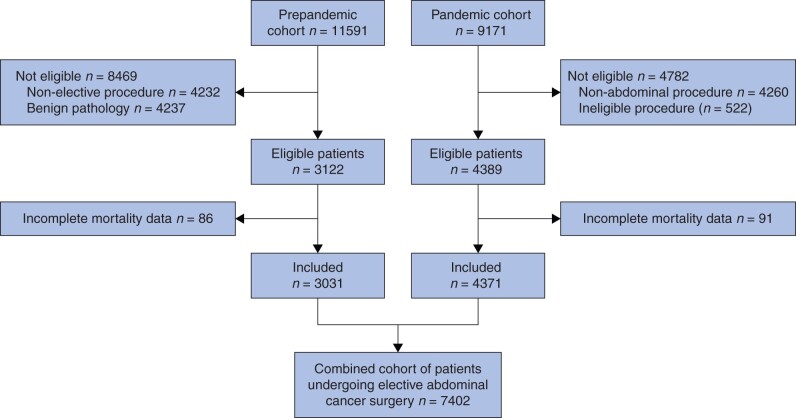
This was a patient-level, comparative analysis of two, international prospective cohort studies: one before the pandemic (January-October 2019) and the second during the SARS-CoV-2 pandemic (local emergence of COVID-19 up to 19 April 2020). Both included patients undergoing elective resection of an intra-abdominal cancer with curative intent across five surgical oncology disciplines. Patient selection and rates of 30-day postoperative pulmonary complications were compared. The primary outcome was 30-day postoperative mortality. Mediation analysis using a natural-effects model was used to estimate the proportion of deaths during the pandemic attributable to SARS-CoV-2 infection.
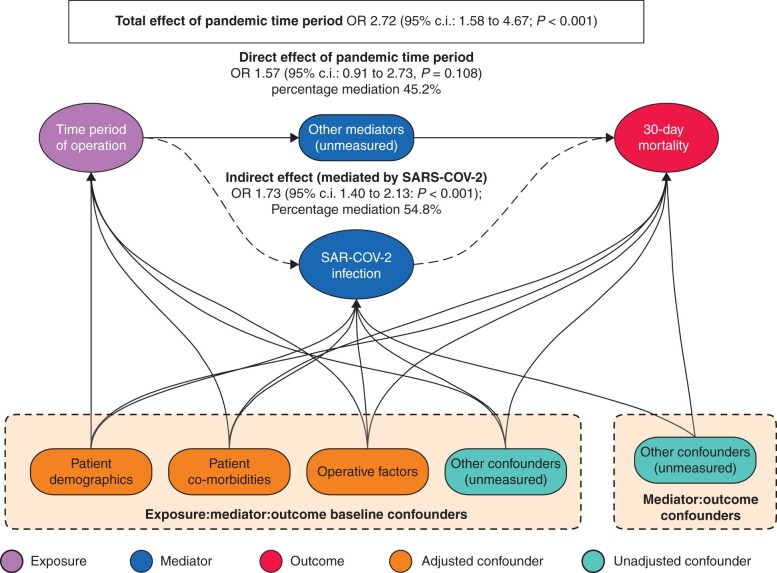
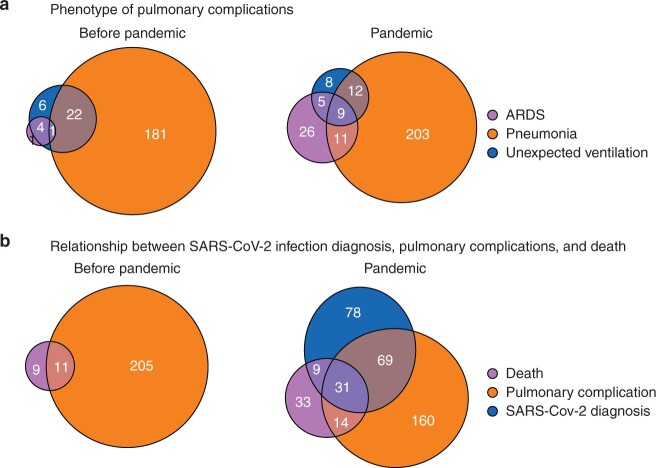
This study included 7402 patients from 50 countries; 3031 (40.9 per cent) underwent surgery before and 4371 (59.1 per cent) during the pandemic. Overall, 4.3 per cent (187 of 4371) developed postoperative SARS-CoV-2 in the pandemic cohort. The pulmonary complication rate was similar (7.1 per cent (216 of 3031) versus 6.3 per cent (274 of 4371); P = 0.158) but the mortality rate was significantly higher (0.7 per cent (20 of 3031) versus 2.0 per cent (87 of 4371); P < 0.001) among patients who had surgery during the pandemic. The adjusted odds of death were higher during than before the pandemic (odds ratio (OR) 2.72, 95 per cent c.i. 1.58 to 4.67; P < 0.001). In mediation analysis, 54.8 per cent of excess postoperative deaths during the pandemic were estimated to be attributable to SARS-CoV-2 (OR 1.73, 1.40 to 2.13; P < 0.001).
Although providers may have selected patients with a lower risk profile for surgery during the pandemic, this did not mitigate the likelihood of death through SARS-CoV-2 infection. Care providers must act urgently to protect surgical patients from SARS-CoV-2 infection.
本研究旨在确定在严重急性呼吸综合征冠状病毒 2 (SARS-CoV-2)大流行前后,肺部并发症对手术死亡的影响。
这是一项患者水平的、比较性的分析,纳入了两项国际前瞻性队列研究:一项在大流行前(2019 年 1 月至 10 月)进行,另一项在 SARS-CoV-2 大流行期间(当地 COVID-19 出现至 2020 年 4 月 19 日)进行。这两项研究均包括五个外科肿瘤学领域接受择期根治性切除腹部癌症的患者。比较了患者选择和 30 天术后肺部并发症的发生率。主要结局是 30 天术后死亡率。使用自然效应模型进行中介分析,以估计大流行期间归因于 SARS-CoV-2 感染的死亡比例。
本研究纳入了来自 50 个国家的 7402 名患者;其中 3031 名(40.9%)在大流行前接受手术,4371 名(59.1%)在大流行期间接受手术。总体而言,大流行期间,在疫情队列中有 4.3%(4371 名中的 187 名)发生了术后 SARS-CoV-2。肺部并发症发生率相似(7.1%(3031 名中的 216 名)与 6.3%(4371 名中的 274 名);P=0.158),但在大流行期间接受手术的患者死亡率明显更高(0.7%(3031 名中的 20 名)与 2.0%(4371 名中的 87 名);P<0.001)。与大流行前相比,大流行期间死亡的调整后比值比更高(比值比(OR)2.72,95%置信区间 1.58 至 4.67;P<0.001)。在中介分析中,估计大流行期间术后过度死亡的 54.8%归因于 SARS-CoV-2(OR 1.73,1.40 至 2.13;P<0.001)。
尽管在大流行期间,医生可能会选择风险较低的患者进行手术,但这并不能减轻 SARS-CoV-2 感染导致的死亡可能性。医护人员必须立即采取行动,保护外科患者免受 SARS-CoV-2 感染。