Department of Cardiac Surgery, Medical University of Innsbruck, Innsbruck, Austria.
Department of Clinical and Functional Anatomy, Medical University of Innsbruck, Innsbruck, Austria.
Interact Cardiovasc Thorac Surg. 2022 Feb 21;34(3):361-368. doi: 10.1093/icvts/ivab330.
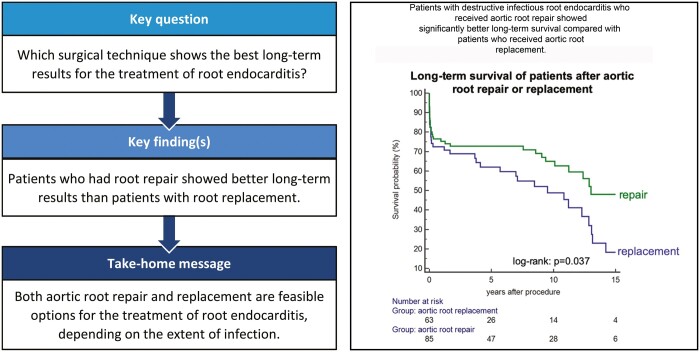
Surgical treatment of destructive infective endocarditis consists of extensive debridement followed by root repair or replacement. However, it remains unknown whether 1 is superior to the other. We aimed to analyse whether long-term results were better after root repair or replacement in patients with root endocarditis.
A total of 148 consecutive patients with root endocarditis treated with surgery from 1997 to 2020 at our department were included. Patients were divided into 2 groups: aortic root repair (n = 85) or root replacement using xenografts or homografts (n = 63).
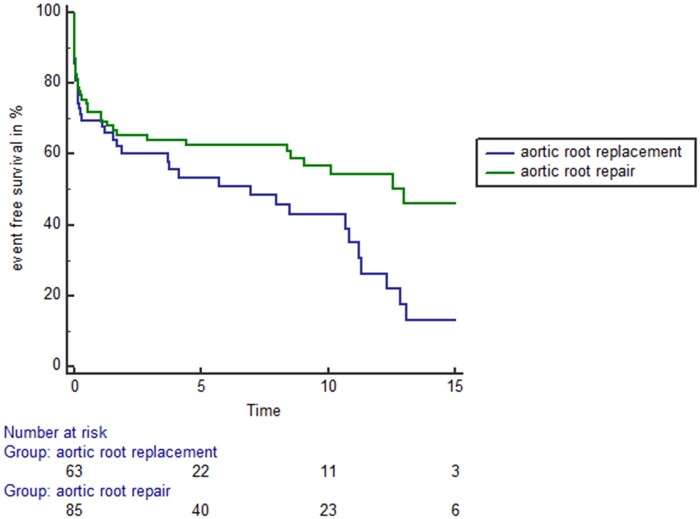
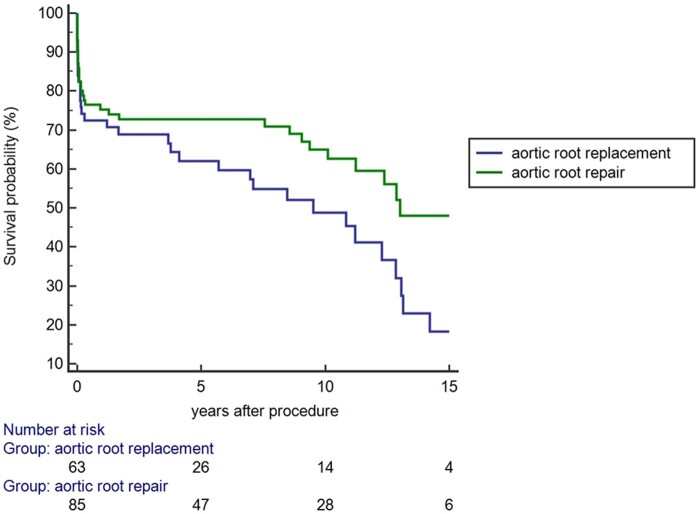
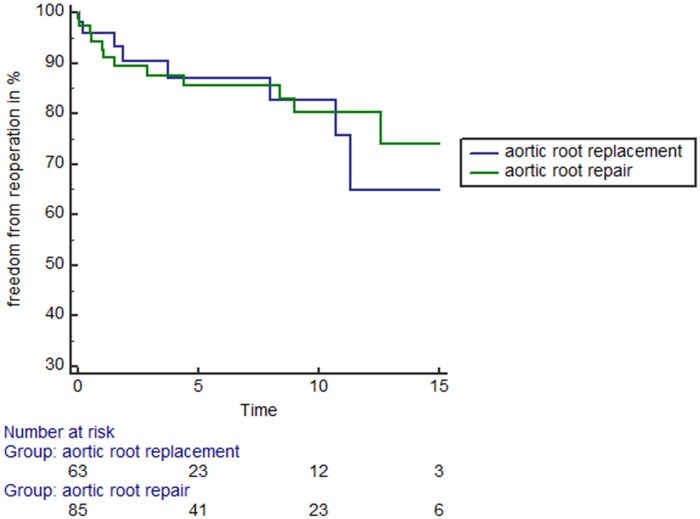
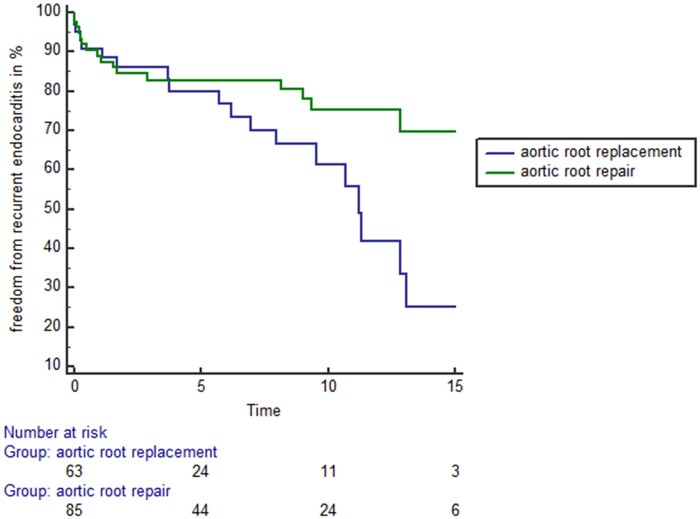
Patients receiving aortic root repair showed significantly better long-term survival compared to patients receiving aortic root replacement (log-rank: P = 0.037). There was no difference in terms of freedom from valvular reoperations among both treatment groups (log-rank: P = 0.58). Patients with aortic root repair showed higher freedom from recurrent endocarditis compared to patients with aortic root replacement (log-rank: P = 0.022). Patients with aortic root repair exhibited higher event-free survival (defined as a combination end point of freedom from death, valvular reoperation or recurrent endocarditis) compared to patients receiving aortic root replacement (log-rank: P = 0.022). Age increased the risk of mortality with 1.7% per year. Multi-variable adjusted statistical analysis revealed improved long-term event-free survival after aortic root repair (hazards ratio: 0.57, 95% confidence interval: 0.39-0.95; P = 0.031).
Aortic root repair and replacement are feasible options for the surgical treatment of root endocarditis and are complementary methods, depending on the extent of infection. Patients with less advanced infection have a more favourable prognosis.
UN4232 382/3.1 (retrospective study).
破坏性感染性心内膜炎的手术治疗包括广泛清创,随后进行根部修复或替换。然而,目前尚不清楚两者之间哪一种更优。我们旨在分析根部心内膜炎患者行根部修复或替换术后的长期结果是否存在差异。
回顾性分析了 1997 年至 2020 年在我科行手术治疗的 148 例连续根部心内膜炎患者。患者分为两组:主动脉根部修复组(n=85)或使用异种移植物或同种移植物行根部替换组(n=63)。
主动脉根部修复组患者的长期生存率明显优于主动脉根部替换组(log-rank:P=0.037)。两组患者在瓣膜再次手术方面无差异(log-rank:P=0.58)。主动脉根部修复组患者的复发性心内膜炎发生率低于主动脉根部替换组(log-rank:P=0.022)。主动脉根部修复组患者的无事件生存率(定义为死亡、瓣膜再次手术或复发性心内膜炎的组合终点)高于主动脉根部替换组(log-rank:P=0.022)。年龄每增加 1 岁,死亡率增加 1.7%。多变量调整后分析显示,主动脉根部修复后长期无事件生存率提高(风险比:0.57,95%置信区间:0.39-0.95;P=0.031)。
主动脉根部修复和替换是治疗根部心内膜炎的可行选择,两者是互补的方法,取决于感染的范围。感染程度较轻的患者预后更有利。
UN4232 382/3.1(回顾性研究)。