Department of Medicine, University of Mississippi School of Medicine, Jackson, MS, USA.
Baylor Heart and Vascular Institute, 621 North Hall Street, Dallas, TX 75226, USA.
Eur Heart J. 2022 Feb 3;43(5):416-426. doi: 10.1093/eurheartj/ehab798.
No therapy has shown to reduce the risk of hospitalization for heart failure across the entire range of ejection fractions seen in clinical practice. We assessed the influence of ejection fraction on the effect of the sodium-glucose cotransporter 2 inhibitor empagliflozin on heart failure outcomes.
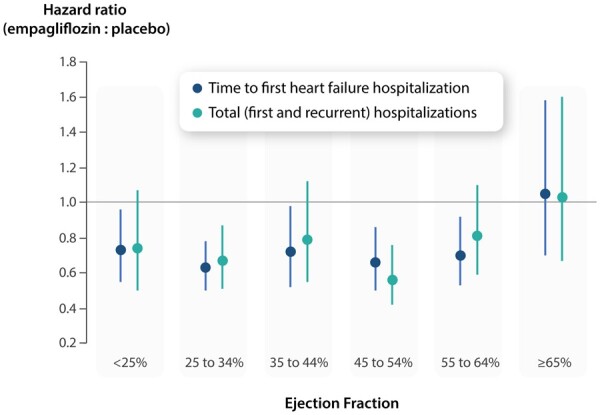
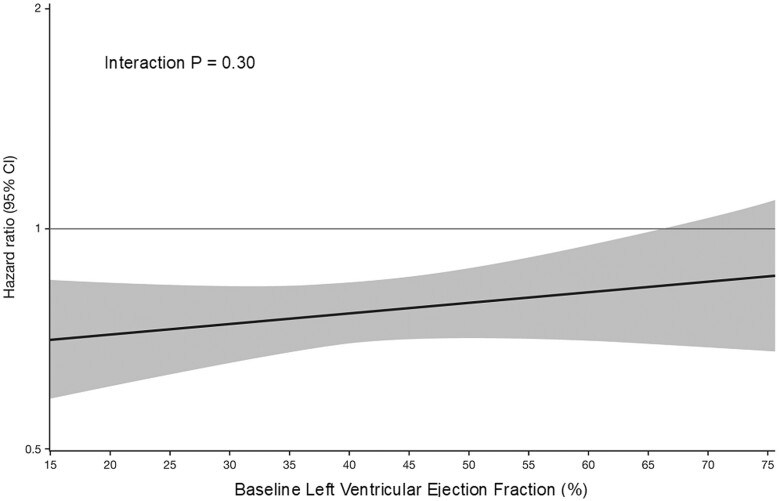
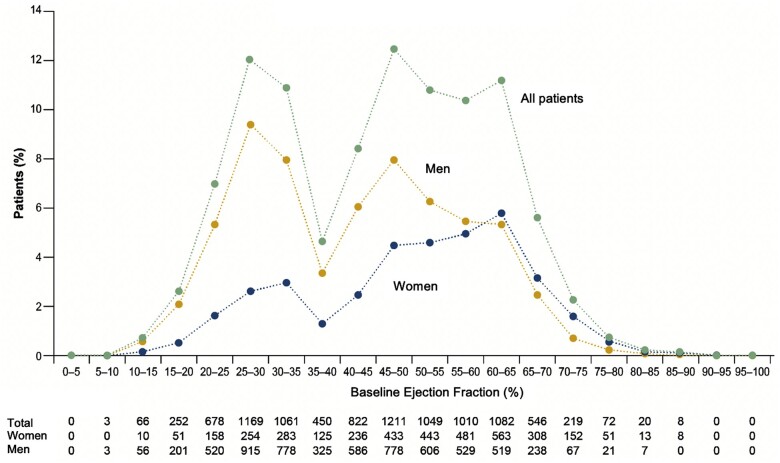
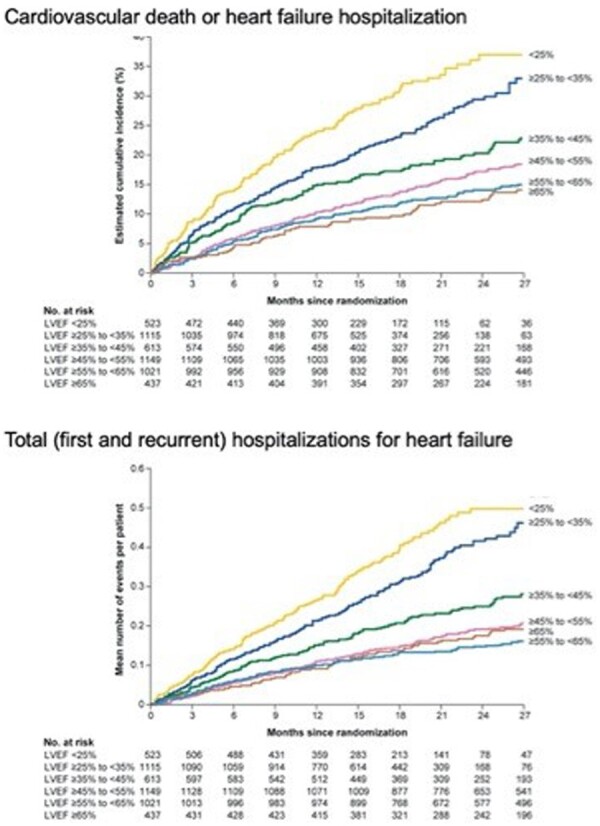
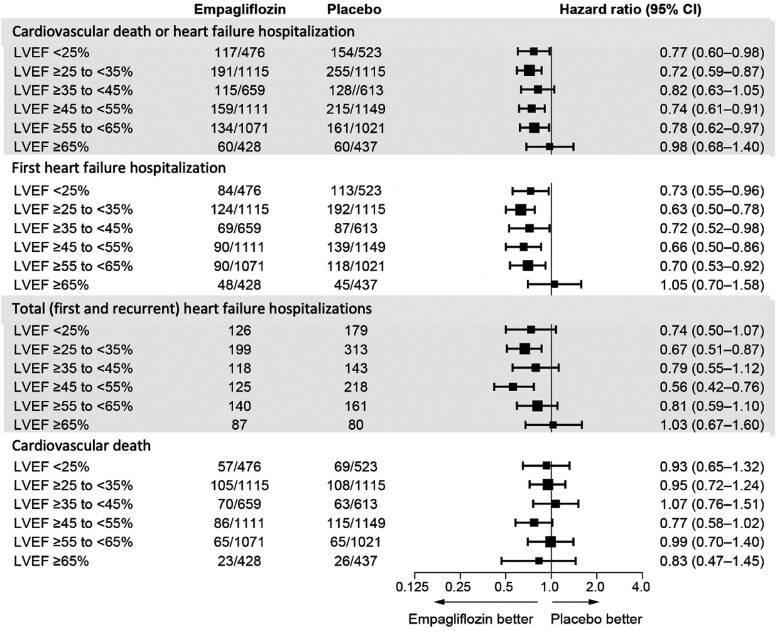
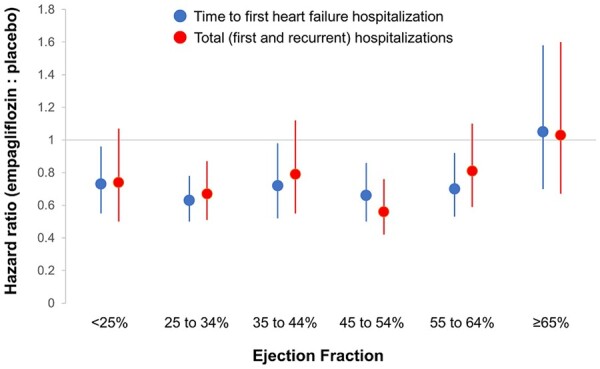
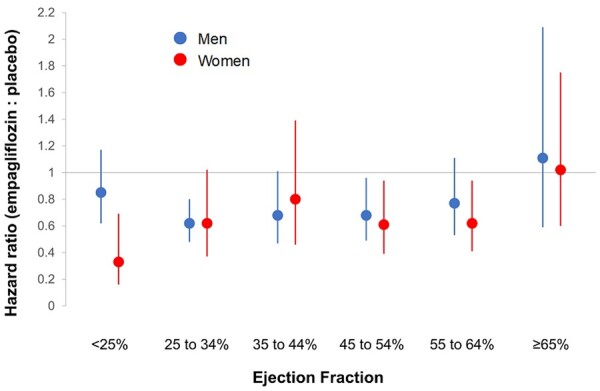
A pooled analysis was performed on both the EMPEROR-Reduced and EMPEROR-Preserved trials (9718 patients; 4860 empagliflozin and 4858 placebo), and patients were grouped based on ejection fraction: <25% (n = 999), 25-34% (n = 2230), 35-44% (n = 1272), 45-54% (n = 2260), 55-64% (n = 2092), and ≥65% (n = 865). Outcomes assessed included (i) time to first hospitalization for heart failure or cardiovascular mortality, (ii) time to first heart failure hospitalization, (iii) total (first and recurrent) hospitalizations for heart failure, and (iv) health status assessed by the Kansas City Cardiomyopathy Questionnaire (KCCQ). The risk of cardiovascular death and hospitalization for heart failure declined progressively as ejection fraction increased from <25% to ≥65%. Empagliflozin reduced the risk of cardiovascular death or heart failure hospitalization, mainly by reducing heart failure hospitalizations. Empagliflozin reduced the risk of heart failure hospitalization by ≈30% in all ejection fraction subgroups, with an attenuated effect in patients with an ejection fraction ≥65%. Hazard ratios and 95% confidence intervals were: ejection fraction <25%: 0.73 (0.55-0.96); ejection fraction 25-34%: 0.63 (0.50-0.78); ejection fraction 35-44%: 0.72 (0.52-0.98); ejection fraction 45-54%: 0.66 (0.50-0.86); ejection fraction 55-64%: 0.70 (0.53-0.92); and ejection fraction ≥65%: 1.05 (0.70-1.58). Other heart failure outcomes and measures, including KCCQ, showed a similar response pattern. Sex did not influence the responses to empagliflozin.
The magnitude of the effect of empagliflozin on heart failure outcomes was clinically meaningful and similar in patients with ejection fractions <25% to <65%, but was attenuated in patients with an ejection fraction ≥65%.
How does ejection fraction influence the effects of empagliflozin in patients with heart failure and either a reduced or a preserved ejection fraction?
The magnitude of the effect of empagliflozin on heart failure outcomes and health status was similar in patients with ejection fractions <25% to <65%, but it was attenuated in patients with an ejection fraction ≥65%.
The consistency of the response in patients with ejection fractions of <25% to <65% distinguishes the effects of empagliflozin from other drugs that have been evaluated across the full spectrum of ejection fractions in patients with heart failure.
在临床实践中观察到的整个射血分数范围内,尚无任何疗法显示可降低心力衰竭住院风险。我们评估了射血分数对钠-葡萄糖共转运蛋白 2 抑制剂恩格列净对心力衰竭结局影响的作用。
对 EMPEROR-Reduced 和 EMPEROR-Preserved 试验(9718 例患者;恩格列净 4860 例,安慰剂 4858 例)进行了汇总分析,并根据射血分数将患者分为以下组:<25%(n=999)、25-34%(n=2230)、35-44%(n=1272)、45-54%(n=2260)、55-64%(n=2092)和≥65%(n=865)。评估的结局包括:(i)首次因心力衰竭或心血管死亡住院的时间,(ii)首次心力衰竭住院时间,(iii)心力衰竭总住院次数(首次和复发),(iv)由堪萨斯城心肌病问卷(KCCQ)评估的健康状况。随着射血分数从<25%增加到≥65%,心血管死亡和心力衰竭住院的风险逐渐降低。恩格列净降低了心血管死亡或心力衰竭住院的风险,主要是通过降低心力衰竭住院的风险。恩格列净降低了所有射血分数亚组中约 30%的心力衰竭住院风险,而在射血分数≥65%的患者中,这种效果减弱。风险比和 95%置信区间为:射血分数<25%:0.73(0.55-0.96);射血分数 25-34%:0.63(0.50-0.78);射血分数 35-44%:0.72(0.52-0.98);射血分数 45-54%:0.66(0.50-0.86);射血分数 55-64%:0.70(0.53-0.92);射血分数≥65%:1.05(0.70-1.58)。其他心力衰竭结局和指标,包括 KCCQ,也显示出类似的反应模式。性别并未影响恩格列净的反应。
恩格列净对心力衰竭结局的影响程度具有临床意义,在射血分数<25%至<65%的患者中效果相似,但在射血分数≥65%的患者中效果减弱。
射血分数如何影响心力衰竭和射血分数降低或保留的患者中恩格列净的作用?
恩格列净对心力衰竭结局和健康状况的影响程度在射血分数<25%至<65%的患者中相似,但在射血分数≥65%的患者中减弱。
射血分数<25%至<65%患者的反应一致性将恩格列净的作用与在心力衰竭患者整个射血分数范围内评估的其他药物区分开来。