Busse David, Simon Philipp, Schmitt Lisa, Petroff David, Dorn Christoph, Dietrich Arne, Zeitlinger Markus, Huisinga Wilhelm, Michelet Robin, Wrigge Hermann, Kloft Charlotte
Department of Clinical Pharmacy and Biochemistry, Institute of Pharmacy, Freie Universitaet Berlin, Kelchstr. 31, 12169, Berlin, Germany.
Graduate Research Training Program PharMetrX, Berlin, Germany.
Clin Pharmacokinet. 2022 May;61(5):655-672. doi: 10.1007/s40262-021-01070-6. Epub 2021 Dec 11.
A quantitative evaluation of the PK of meropenem, a broad-spectrum β-lactam antibiotic, in plasma and interstitial space fluid (ISF) of subcutaneous adipose tissue of obese patients is lacking as of date. The objective of this study was the characterisation of meropenem population pharmacokinetics in plasma and ISF in obese and non-obese patients for identification of adequate dosing regimens via Monte-Carlo simulations.
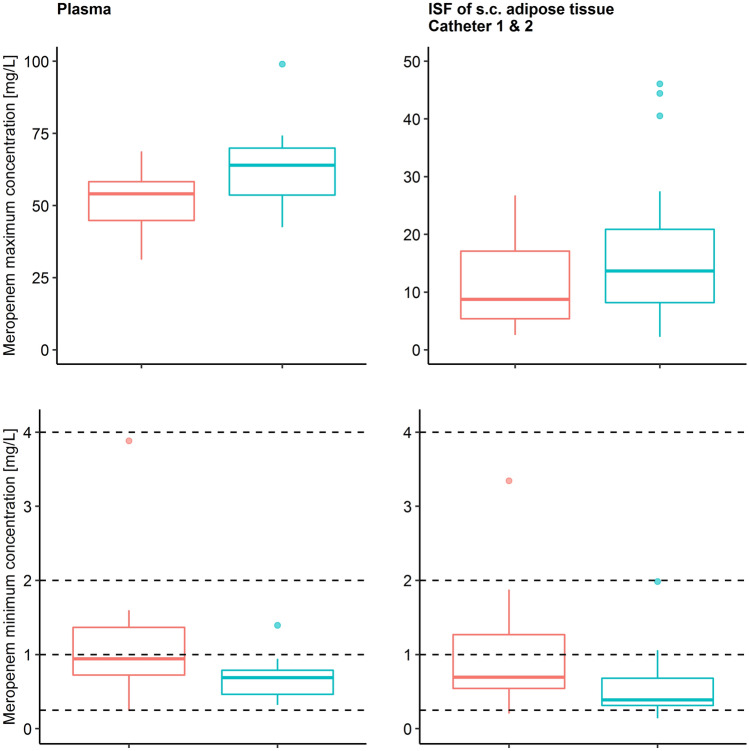
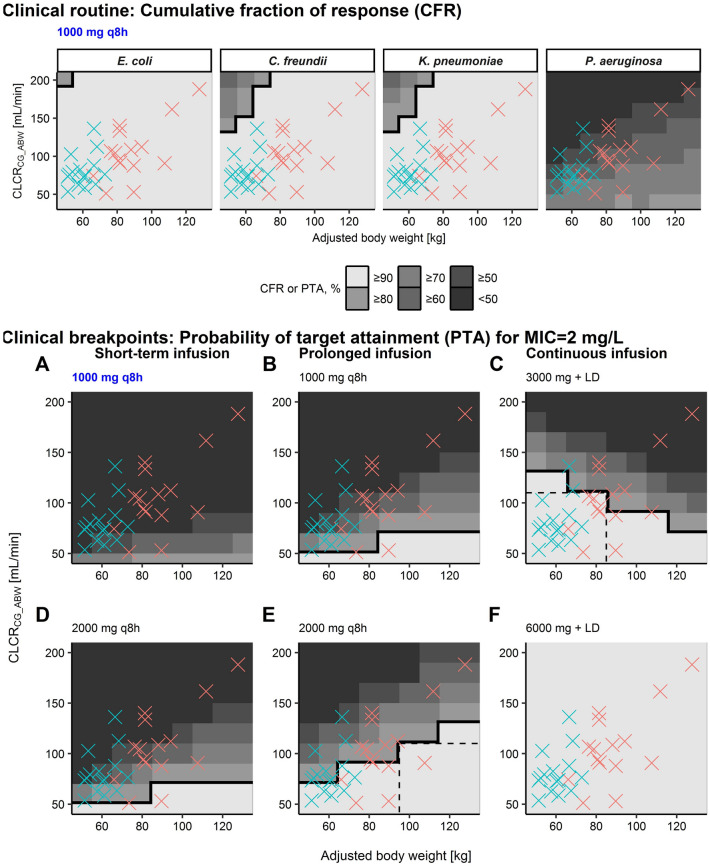
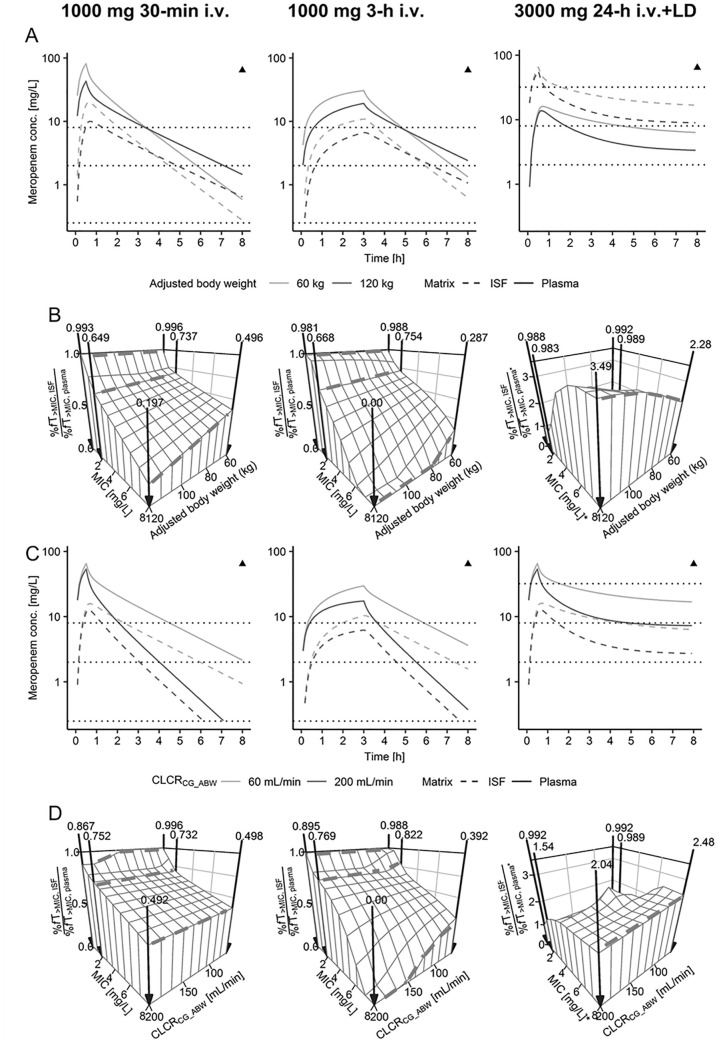
We obtained plasma and microdialysate concentrations after administration of meropenem 1000 mg to 15 obese and 15 non-obese surgery patients from a prospective clinical trial. After characterizing plasma- and microdialysis-derived ISF pharmacokinetics via population pharmacokinetic analysis, we simulated thrice-daily (TID) meropenem short-term (0.5 h), prolonged (3.0 h), and continuous infusions. Adequacy of therapy was assessed by the probability of pharmacokinetic/pharmacodynamic (PK/PD) target attainment (PTA) analysis based on time unbound concentrations exceeded minimum inhibitory concentrations (MIC) on treatment day 1 (%fT) and the sum of PTA weighted by relative frequency of MIC values for infections by pathogens commonly treated with meropenem. To avoid interstitial tissue fluid concentrations below MIC for the entire dosing interval during continuous infusions, a more conservative PK/PD index was selected (%fT).
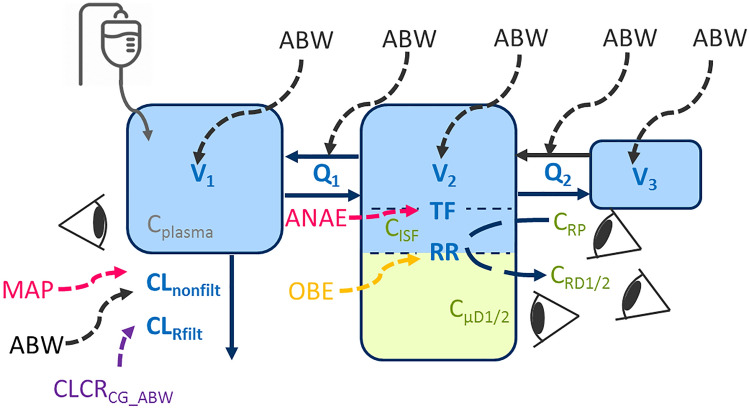
Adjusted body weight (ABW) and calculated creatinine clearance (CLCR) of all patients (body mass index [BMI] = 20.5-81.5 kg/m) explained a considerable proportion of the between-patient pharmacokinetic variability (15.1-31.0% relative reduction). The ISF:plasma ratio of %fT was relatively similar for MIC ≤ 2 mg/L but decreased for MIC = 8 mg/L over ABW = 60-120 kg (0.50-0.20). Steady-state concentrations were 2.68 times (95% confidence interval [CI] = 2.11-3.37) higher in plasma than in ISF, supporting PK/PD targets related to four times the MIC during continuous infusions to avoid suspected ISF concentrations constantly below the MIC. A 3000 mg/24 h continuous infusion was sufficient at MIC = 2 mg/L for patients with CLCR ≤ 100 mL/min and ABW < 90 kg, whereas 2000 mg TID prolonged infusions were adequate for those with CLCR ≤ 100 mL/min and ABW > 90 kg. For MIC = 2 mg/L and %fT = 95, PTA was adequate in patients over the entire investigated range of body mass and renal function using a 6000 mg continuous infusion. A prolonged infusion of meropenem 2000 mg TID was sufficient for MIC ≤ 8 mg/L and all investigated ABW and CLCR when employing the PK/PD target %fT = 40. Short-term infusions of 1000 mg TID were sufficient for CLCR ≤ 130 mL/min and distributions of MIC values for Escherichia coli, Citrobacter freundii, and Klebsiella pneumoniae but not for Pseudomonas aeruginosa.
This analysis indicated a need for higher doses (≥ 2000 mg) and prolonged infusions (≥ 3 h) for obese and non-obese patients at MIC ≥ 2 mg/L. Higher PTA was achieved with prolonged infusions in obese patients and with continuous infusions in non-obese patients.
EudraCT: 2012-004383-22.
迄今为止,缺乏对肥胖患者皮下脂肪组织血浆和组织间隙液(ISF)中广谱β-内酰胺抗生素美罗培南的药代动力学(PK)进行定量评估。本研究的目的是表征肥胖和非肥胖患者血浆和ISF中美罗培南的群体药代动力学,通过蒙特卡洛模拟确定合适的给药方案。
我们从一项前瞻性临床试验中获取了15名肥胖和15名非肥胖手术患者静脉注射1000mg美罗培南后的血浆和微透析液浓度。通过群体药代动力学分析对血浆和微透析衍生的ISF药代动力学进行表征后,我们模拟了美罗培南每日三次(TID)的短期(0.5小时)、延长(3.0小时)和持续输注。基于治疗第1天超过最低抑菌浓度(MIC)的游离时间浓度(%fT)以及美罗培南通常治疗的病原体感染的MIC值相对频率加权的PTA分析,评估治疗的充分性。为避免持续输注期间整个给药间隔内组织间隙液浓度低于MIC,选择了更保守的PK/PD指数(%fT)。
所有患者(体重指数[BMI]=20.5-81.5kg/m²)的校正体重(ABW)和计算的肌酐清除率(CLCR)解释了相当一部分患者间药代动力学变异性(相对降低15.1-31.0%)。对于MIC≤2mg/L,ISF:血浆的%fT比值相对相似,但对于MIC=8mg/L,ABW=60-120kg时该比值降低(0.50-0.20)。稳态浓度在血浆中比在ISF中高2.68倍(95%置信区间[CI]=2.11-3.37),这支持了持续输注期间与四倍MIC相关的PK/PD目标,以避免疑似ISF浓度持续低于MIC。对于CLCR≤100mL/min且ABW<90kg的患者,MIC=2mg/L时24小时持续输注3000mg就足够了,而对于CLCR≤100mL/min且ABW>90kg的患者,每日三次延长输注2000mg就足够了。对于MIC=2mg/L和%fT=95,使用6000mg持续输注时,在整个研究的体重和肾功能范围内患者的PTA是足够的。当采用PK/PD目标%fT=40时,每日三次延长输注2000mg美罗培南对于MIC≤8mg/L以及所有研究的ABW和CLCR都是足够的。对于CLCR≤130mL/min以及大肠杆菌、弗氏柠檬酸杆菌和肺炎克雷伯菌的MIC值分布情况,每日三次短期输注1000mg是足够的,但对于铜绿假单胞菌则不够。
该分析表明,对于MIC≥2mg/L的肥胖和非肥胖患者,需要更高剂量(≥2000mg)和延长输注时间(≥3小时)。肥胖患者延长输注以及非肥胖患者持续输注可实现更高的PTA。
EudraCT:2012-004383-22。