Coleman Jesse, Ginsburg Amy Sarah, Macharia William M, Ochieng Roseline, Zhou Guohai, Dunsmuir Dustin, Karlen Walter, Ansermino J Mark
Evaluation of Technologies for Neonates in Africa (ETNA), Aga Khan University Hospital, Nairobi, Kenya.
University of Washington, Seattle, WA, 98195, USA.
Gates Open Res. 2021 Oct 8;5:93. doi: 10.12688/gatesopenres.13237.2. eCollection 2021.
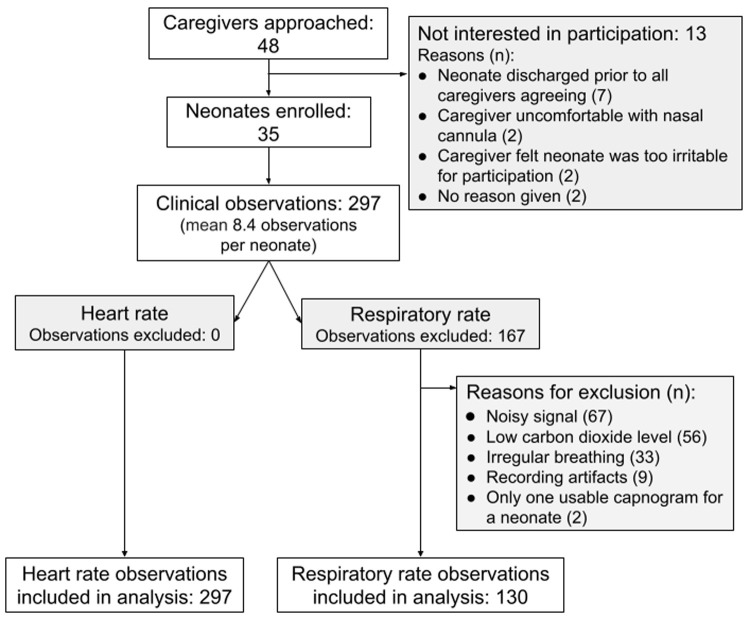
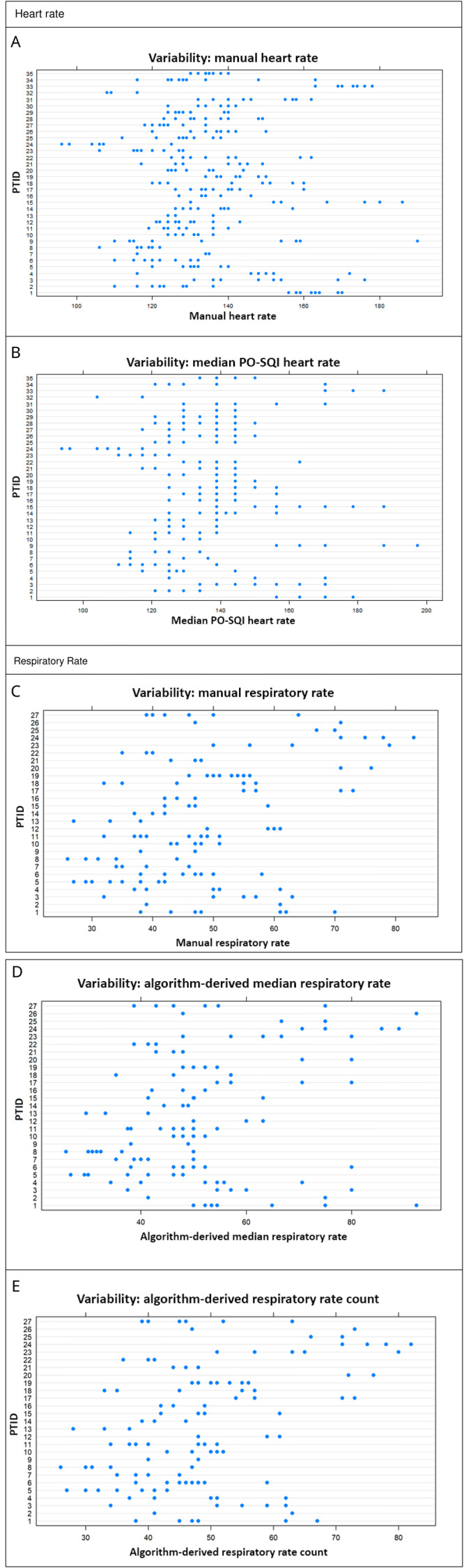
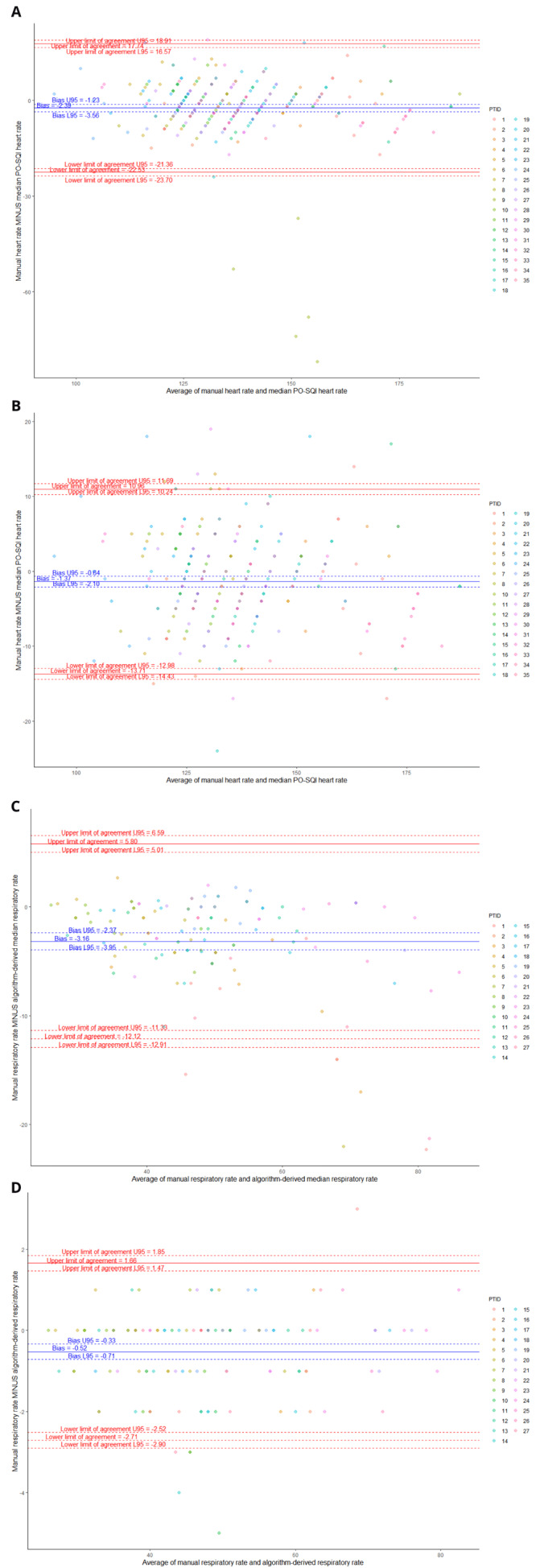
Heart rate (HR) and respiratory rate (RR) can be challenging to measure accurately and reliably in neonates. The introduction of innovative, non-invasive measurement technologies suitable for resource-constrained settings is limited by the lack of appropriate clinical thresholds for accuracy comparison studies. We collected measurements of photoplethysmography-recorded HR and capnography-recorded exhaled carbon dioxide across multiple 60-second epochs (observations) in enrolled neonates admitted to the neonatal care unit at Aga Khan University Hospital in Nairobi, Kenya. Trained study nurses manually recorded HR, and the study team manually counted individual breaths from capnograms. For comparison, HR and RR also were measured using an automated signal detection algorithm. Clinical measurements were analyzed for repeatability. A total of 297 epochs across 35 neonates were recorded. Manual HR showed a bias of -2.4 (-1.8%) and a spread between the 95% limits of agreement (LOA) of 40.3 (29.6%) compared to the algorithm-derived median HR. Manual RR showed a bias of -3.2 (-6.6%) and a spread between the 95% LOA of 17.9 (37.3%) compared to the algorithm-derived median RR, and a bias of -0.5 (1.1%) and a spread between the 95% LOA of 4.4 (9.1%) compared to the algorithm-derived RR count. Manual HR and RR showed repeatability of 0.6 (interquartile range (IQR) 0.5-0.7), and 0.7 (IQR 0.5-0.8), respectively. Appropriate clinical thresholds should be selected when performing accuracy comparisons for HR and RR. Automated measurement technologies typically use a smoothing or averaging filter, which significantly impacts accuracy. A wider spread between the LOA, as much as 30%, should be considered to account for the observed physiological nuances and within- and between-neonate variability and different averaging methods. Wider adoption of thresholds by data standards organizations and technology developers and manufacturers will increase the robustness of clinical comparison studies.
在新生儿中,准确可靠地测量心率(HR)和呼吸频率(RR)具有挑战性。由于缺乏用于准确性比较研究的适当临床阈值,适用于资源有限环境的创新型非侵入性测量技术的引入受到限制。我们收集了肯尼亚内罗毕阿迦汗大学医院新生儿护理病房收治的新生儿在多个60秒时间段(观察期)内通过光电容积脉搏波描记法记录的心率和通过二氧化碳描记法记录的呼出二氧化碳的数据。经过培训的研究护士手动记录心率,研究团队从二氧化碳图中手动计数个体呼吸次数。为作比较,心率和呼吸频率也使用自动信号检测算法进行测量。对临床测量结果进行了重复性分析。共记录了35名新生儿的297个时间段的数据。与算法得出的心率中位数相比,手动记录的心率偏差为-2.4(-1.8%),95%一致性界限(LOA)之间的差值为40.3(29.6%)。与算法得出的呼吸频率中位数相比,手动记录的呼吸频率偏差为-3.2(-6.6%),95% LOA之间的差值为17.9(37.3%),与算法得出的呼吸次数相比,偏差为-0.5(1.1%),95% LOA之间的差值为4.4(9.1%)。手动记录的心率和呼吸频率的重复性分别为0.6(四分位间距(IQR)0.5 - 0.7)和0.7(IQR 0.5 - 0.8)。在对心率和呼吸频率进行准确性比较时,应选择适当的临床阈值。自动测量技术通常使用平滑或平均滤波器,这会显著影响准确性。应考虑LOA之间更宽的差值,高达30%,以解释观察到的生理细微差别以及新生儿内部和之间的变异性以及不同的平均方法。数据标准组织以及技术开发者和制造商更广泛地采用这些阈值将提高临床比较研究的稳健性。