The Parker Institute, Copenhagen University Hospital, Bispebjerg and Frederiksberg, Copenhagen, Denmark
Rheumatology Section, Pontifical Catholic University, School of Medicine, Porto Alegre, Brazil.
Ann Rheum Dis. 2022 Feb;81(2):225-231. doi: 10.1136/annrheumdis-2021-221019. Epub 2021 Dec 15.
To evaluate risankizumab, a biological therapy that inhibits interleukin 23, in patients with active psoriatic arthritis (PsA) who have responded inadequately or are intolerant to ≥1 conventional synthetic disease-modifying antirheumatic drug (csDMARD).
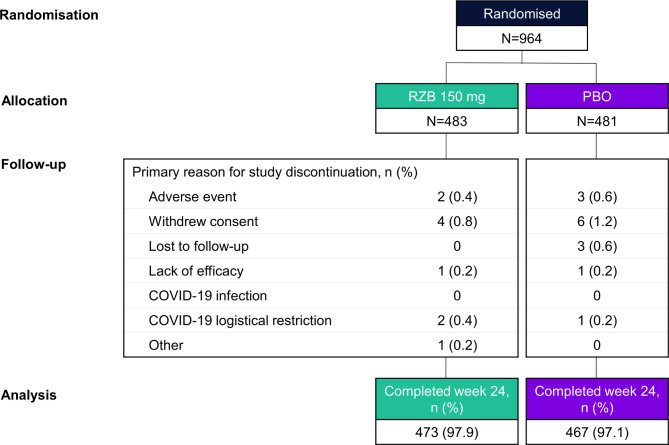
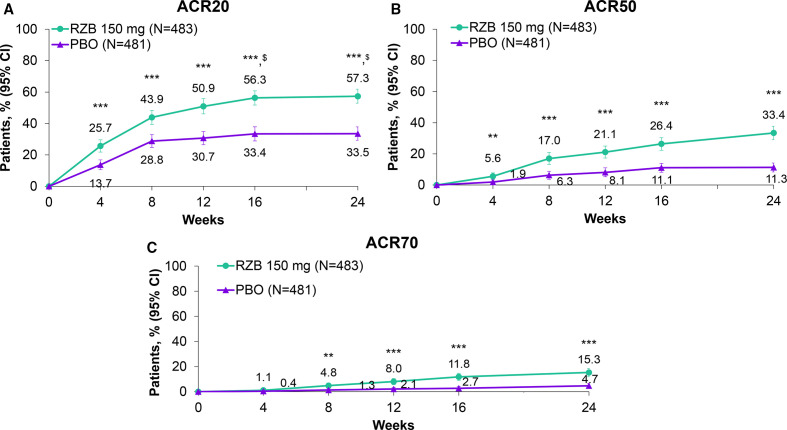
In the randomised, placebo-controlled, double-blind KEEPsAKE 1 trial, 964 patients with active PsA were randomised (1:1) to receive risankizumab 150 mg or placebo at weeks 0, 4 and 16. The primary endpoint was the proportion of patients achieving ≥20% improvement in American College of Rheumatology criteria (ACR20) at week 24. Here, we report the results from the 24-week double-blind period; the open-label period with all patients receiving risankizumab is ongoing.
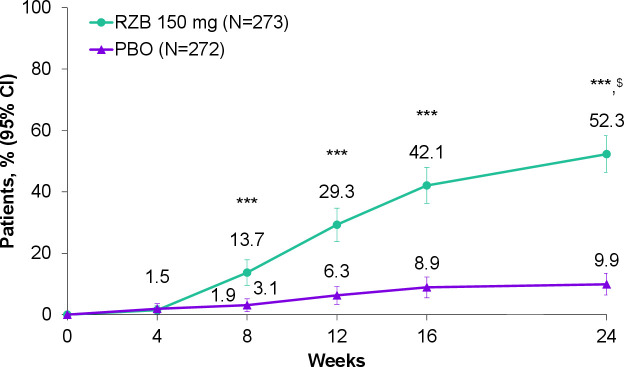
At week 24, a significantly greater proportion of patients receiving risankizumab achieved the primary endpoint of ACR20 (57.3% vs placebo, 33.5%; p<0.001). Significant differences were also observed for risankizumab versus placebo for the first eight ranked secondary endpoints, including skin and nail psoriasis endpoints, minimal disease activity and resolution of enthesitis and dactylitis (p<0.001). Adverse events and serious adverse events were reported at similar rates in the risankizumab and placebo groups. Serious infections were reported for 1.0% and 1.2% of patients receiving risankizumab and placebo, respectively. There was one death in the risankizumab group (urosepsis deemed unrelated to the study drug).
Risankizumab treatment results in significantly greater improvement of signs and symptoms of PsA compared with placebo and is well tolerated in patients with active PsA who have responded inadequately or are intolerant to ≥1 csDMARD.
NCT03675308.
评估 risankizumab,一种抑制白细胞介素 23 的生物疗法,用于治疗对至少 1 种传统合成疾病修饰抗风湿药物(csDMARD)反应不足或不耐受的活动性银屑病关节炎(PsA)患者。
在随机、安慰剂对照、双盲 KEEPsAKE 1 试验中,964 例活动性 PsA 患者按 1:1 比例随机(1:1)接受 risankizumab 150mg 或安慰剂,分别在第 0、4 和 16 周给药。主要终点是第 24 周时达到美国风湿病学会标准(ACR20)改善≥20%的患者比例。在此,我们报告了 24 周双盲期的结果;所有患者正在接受 risankizumab 的开放标签期仍在继续。
在第 24 周时,接受 risankizumab 治疗的患者达到主要终点 ACR20 的比例显著更高(57.3%vs 安慰剂组,33.5%;p<0.001)。与安慰剂相比,risankizumab 还显著改善了前 8 个次要终点,包括皮肤和指甲银屑病终点、最小疾病活动度和附着点炎和指(趾)炎的缓解(p<0.001)。risankizumab 组和安慰剂组报告的不良反应和严重不良反应发生率相似。risankizumab 组和安慰剂组分别有 1.0%和 1.2%的患者报告发生严重感染。risankizumab 组有 1 例死亡(脓毒症被认为与研究药物无关)。
与安慰剂相比,risankizumab 治疗可显著改善 PsA 的体征和症状,并且在对至少 1 种 csDMARD 反应不足或不耐受的活动性 PsA 患者中具有良好的耐受性。
NCT03675308。