Riva Letizia, Casella Gianni, Simonetti Luigi, Zini Andrea
Cardiology Department, Maggiore Hospital, Bologna 40133, Italy.
Neuroradiology Department, Maggiore Hospital, Bologna 40133, Italy.
Eur Heart J Case Rep. 2021 Oct 28;5(11):ytab425. doi: 10.1093/ehjcr/ytab425. eCollection 2021 Nov.
Neurogenic pulmonary oedema (NPO) and Takotsubo cardiomyopathy are rare complications of ischaemic stroke. They are considered to be due to an excess catecholamine release after sympathetic nervous stimulation following stroke onset. Among the different types of Takotsubo cardiomyopathy, apical ballooning is recognized as the typical form, but three atypical patterns have been described (midventricular, basal, and focal) which are more commonly observed in patients with neurological disorders.
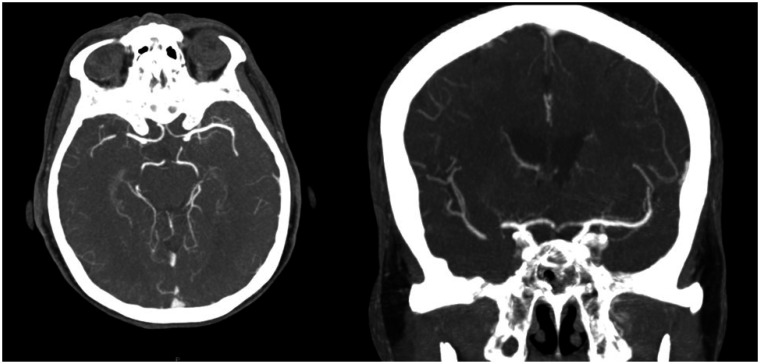
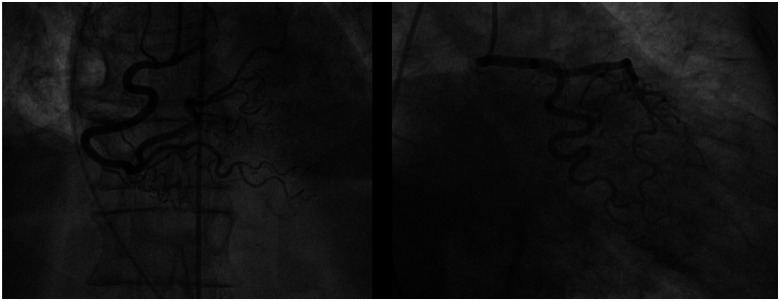
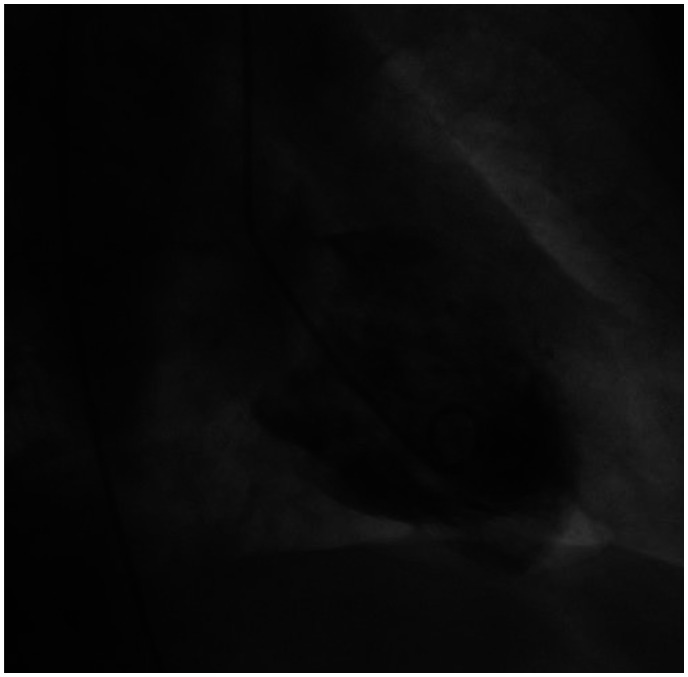
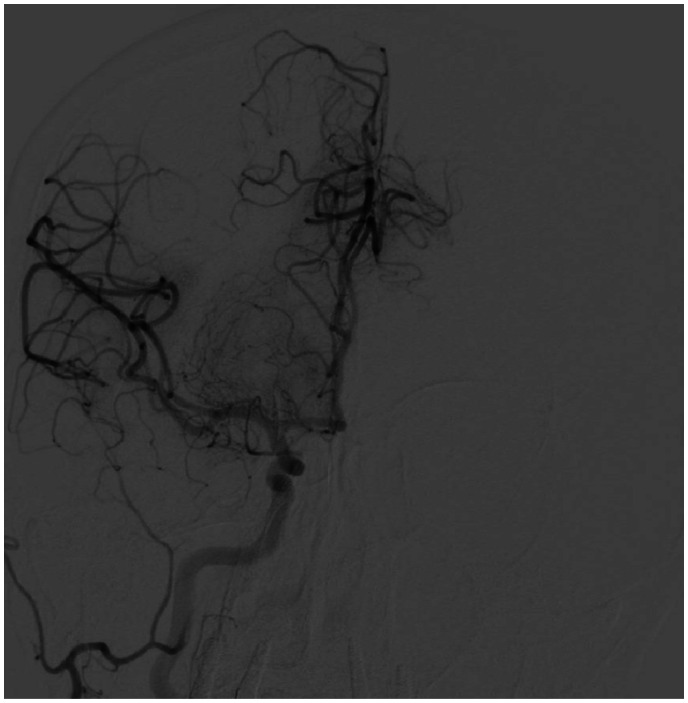
A 78-year-old woman was treated with intravenous alteplase and underwent mechanical thrombectomy for ischaemic stroke. During the procedure, her respiratory condition quickly worsened requiring invasive mechanical ventilation because of a wide and persistent reduction of the inspiratory oxygen fraction/arterial partial oxygen pressure ratio. Transthoracic echocardiography revealed moderate left ventricular systolic dysfunction with akinesis of the septal-apical and inferior-apical segments. Coronary angiography excluded obstructive lesions and/or evidence of acute plaque rupture. Ventriculography confirmed akinesis/dyskinesis of the inferior segment of the left ventricular apex associated with normal kinesis of the remaining segments. Chest X-ray revealed an infiltrative shadow on both lungs. After 24 h from NPO onset, her respiratory function improved and she was finally discharged on Day 7 without neurological defects. Left ventricular systolic dysfunction was reversible and ejection fraction normalized in 3 months.
It is a very rare case of simultaneous NPO and Takotsubo cardiomyopathy following ischaemic stroke. Moreover, it is unique in that it is the first observation of NPO associated with an atypical pattern of Takotsubo cardiomyopathy, which is more frequent in patients with neurological disorders. A rapid recognition and treatment are essential for patient survival.
神经源性肺水肿(NPO)和应激性心肌病是缺血性卒中的罕见并发症。它们被认为是由于卒中发作后交感神经刺激导致儿茶酚胺释放过多所致。在不同类型的应激性心肌病中,心尖气球样变被认为是典型形式,但已描述了三种非典型模式(心室中部、基底和局灶性),这些模式在神经系统疾病患者中更常见。
一名78岁女性因缺血性卒中接受静脉注射阿替普酶治疗并接受了机械取栓术。在手术过程中,由于吸气氧分数/动脉血氧分压比值广泛且持续降低,她的呼吸状况迅速恶化,需要进行有创机械通气。经胸超声心动图显示左心室中度收缩功能障碍,室间隔心尖段和下壁心尖段运动减弱。冠状动脉造影排除了阻塞性病变和/或急性斑块破裂的证据。心室造影证实左心室心尖下壁段运动减弱/运动障碍,其余节段运动正常。胸部X线显示双肺有浸润影。NPO发作24小时后,她的呼吸功能改善,最终在第7天出院,无神经功能缺损。左心室收缩功能障碍是可逆的,射血分数在3个月内恢复正常。
这是一例缺血性卒中后同时发生NPO和应激性心肌病的非常罕见的病例。此外,它的独特之处在于这是首次观察到NPO与应激性心肌病的非典型模式相关,这种模式在神经系统疾病患者中更常见。快速识别和治疗对患者的生存至关重要。