Abi Jaoude Joseph, Thunshelle Connor P, Kouzy Ramez, Nguyen Nicholas D, Lin Daniel, Prakash Laura, Bumanlag Isabela M, Noticewala Sonal S, Niedzielski Joshua S, Beddar Sam, Ludmir Ethan B, Holliday Emma B, Das Prajnan, Minsky Bruce D, Herman Joseph M, Katz Matthew, Koong Albert C, Koay Eugene J, Taniguchi Cullen M
Department of Radiation Oncology, The University of Texas MD Anderson Cancer Center, Houston, Texas.
Department of Radiation Oncology, Radiation Medicine, Zucker School of Medicine at Hofstra/Northwell, Lake Success, Hempstead, New York.
Adv Radiat Oncol. 2021 Jul 29;6(6):100763. doi: 10.1016/j.adro.2021.100763. eCollection 2021 Nov-Dec.
Patients with pancreatic cancer often receive radiation therapy before undergoing surgical resection. We compared the clinical outcomes differences between stereotactic body radiation therapy (SBRT) and 3-dimensional (3D)/intensity-modulated radiation therapy (IMRT).
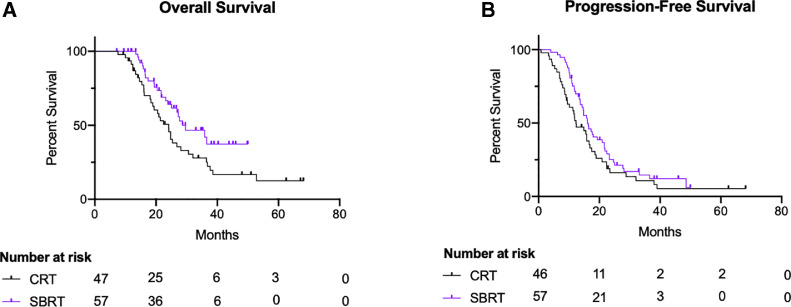
We retrospectively collected data from the University of Texas MD Anderson Cancer Center. Patients with borderline resectable/potentially resectable or locally advanced pancreatic cancer receiving neoadjuvant SBRT (median, 36.0 Gy/5fx), 3D conformal radiation (median, 50.4 Gy/28 fx) or IMRT (median, 50.4 Gy/28 fx) were included. Overall survival (OS) and progression-free survival were analyzed using Cox regression.
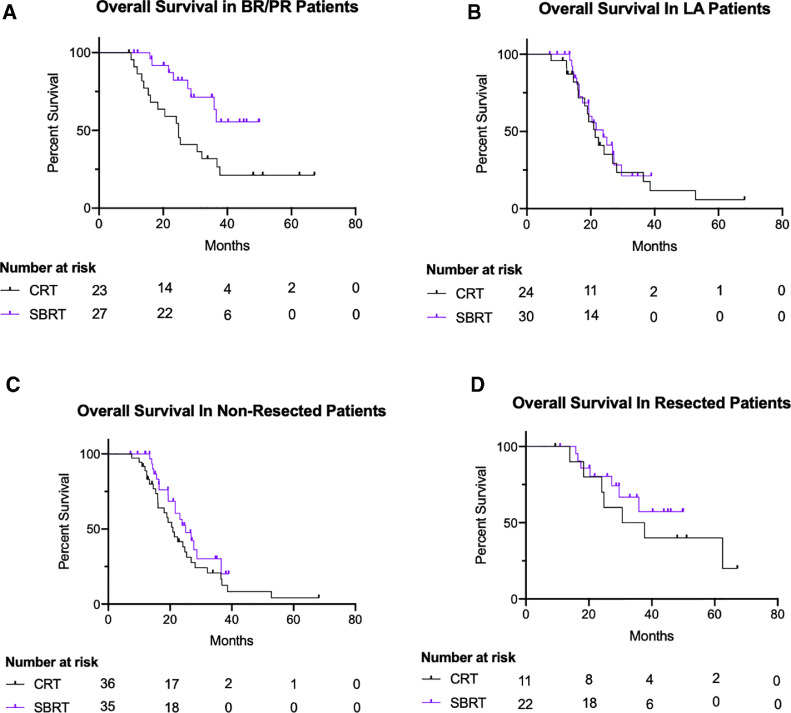
In total, 104 patients were included in our study. Fifty-seven patients (54.8%) were treated with SBRT, and 47 patients (45.2%) were treated with 3D/IMRT. Patients in the SBRT group were slightly older (median age: 70.3 vs 62.7 in the 3D/IMRT group). Both groups had similar proportions of patients with locally advanced pancreatic cancer (SBRT: 30, 52.6%; 3D/IMRT: 24, 51.1%). All patients were treated with chemotherapy. Patients in the SBRT group underwent more surgical resection compared with the 3D/IMRT group (38.6% vs 23.4%, respectively). At a median follow-up of 22 months, a total of 60 patients (57.7%) died: 25 (25/57, 43.9%) in the SBRT group, and 35 (35/47, 74.5%) in the 3D/IMRT group. Median OS was slightly higher in the SBRT group (29.6 months vs 24.1 months in the 3D/IMRT group). On multivariable Cox regression, the choice of radiation therapy technique was not associated with differences in OS (adjusted hazard ratios [aHR] = 0.5; 95% confidence interval [CI], 0.2%-1.3%, = .18). Moreover, patients that underwent surgical resection had better OS (aHR = 0.3, 95% CI, 0.1%-0.8%, = .01). Furthermore, progression-free survival was also similar between patients treated with SBRT and those treated with 3D/IMRT (aHR = 0.9, 95% CI, 0.5%-1.8%, = .81).
SBRT was associated with similar clinical outcomes compared with conventional radiation techniques, despite being delivered over a shorter period of time which would spare patients prolonged treatment burden. Future prospective data are still needed to better assess the role of SBRT in patients with pancreatic cancer.
胰腺癌患者在接受手术切除前常接受放射治疗。我们比较了立体定向体部放射治疗(SBRT)与三维(3D)/调强放射治疗(IMRT)的临床结果差异。
我们回顾性收集了德克萨斯大学MD安德森癌症中心的数据。纳入接受新辅助SBRT(中位剂量,36.0 Gy/5次分割)、3D适形放疗(中位剂量,50.4 Gy/28次分割)或IMRT(中位剂量,50.4 Gy/28次分割)的临界可切除/潜在可切除或局部晚期胰腺癌患者。使用Cox回归分析总生存期(OS)和无进展生存期。
我们的研究共纳入104例患者。57例患者(54.8%)接受了SBRT治疗,47例患者(45.2%)接受了3D/IMRT治疗。SBRT组患者年龄稍大(中位年龄:70.3岁,而3D/IMRT组为62.7岁)。两组局部晚期胰腺癌患者比例相似(SBRT组:30例,52.6%;3D/IMRT组:24例,51.1%)。所有患者均接受了化疗。与3D/IMRT组相比,SBRT组接受手术切除的患者更多(分别为38.6%和23.4%)。在中位随访22个月时,共有60例患者(57.7%)死亡:SBRT组25例(25/57,43.9%),3D/IMRT组35例(35/47,74.5%)。SBRT组的中位OS略高(29.6个月,而3D/IMRT组为24.1个月)。在多变量Cox回归分析中,放射治疗技术的选择与OS差异无关(调整后风险比[aHR]=0.5;95%置信区间[CI],0.2%-1.3%,P=.18)。此外,接受手术切除的患者OS更好(aHR=0.3,95%CI,0.1%-0.8%,P=.OI)。此外,SBRT治疗的患者与3D/IMRT治疗的患者的无进展生存期也相似(aHR=0.9,95%CI,0.5%-1.8%,P=.81)。
与传统放射技术相比,SBRT的临床结果相似,尽管其治疗时间较短,可减轻患者的长期治疗负担。仍需要未来的前瞻性数据来更好地评估SBRT在胰腺癌患者中的作用。