Department of Medical Sciences, Surgery and Neurosciences University of Siena Italy.
Cardiology Intensive Therapy Unit Department of Internal Medicine Nuovo Ospedale San Giovanni di Dio Florence Italy.
J Am Heart Assoc. 2022 Jan 4;11(1):e023371. doi: 10.1161/JAHA.121.023371. Epub 2021 Dec 22.
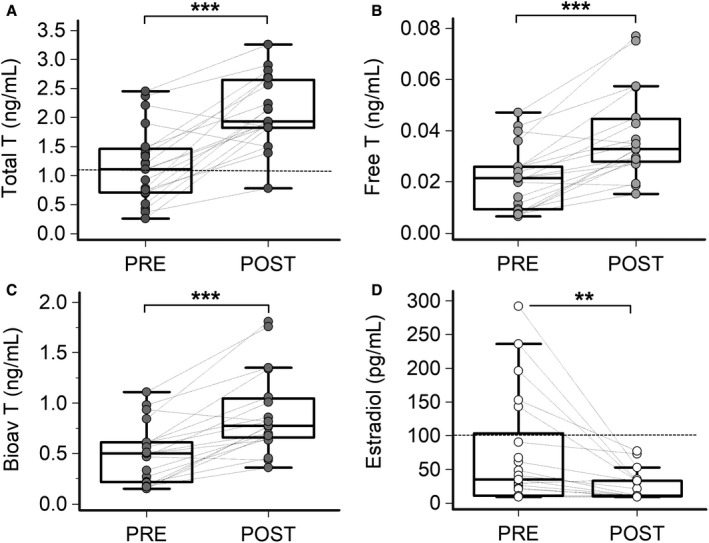
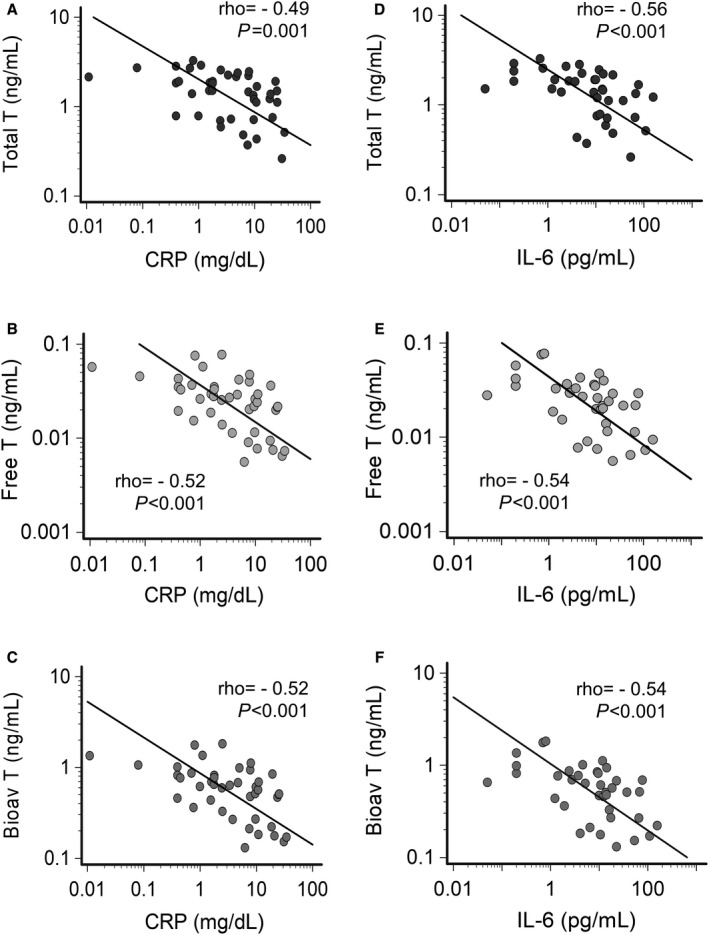
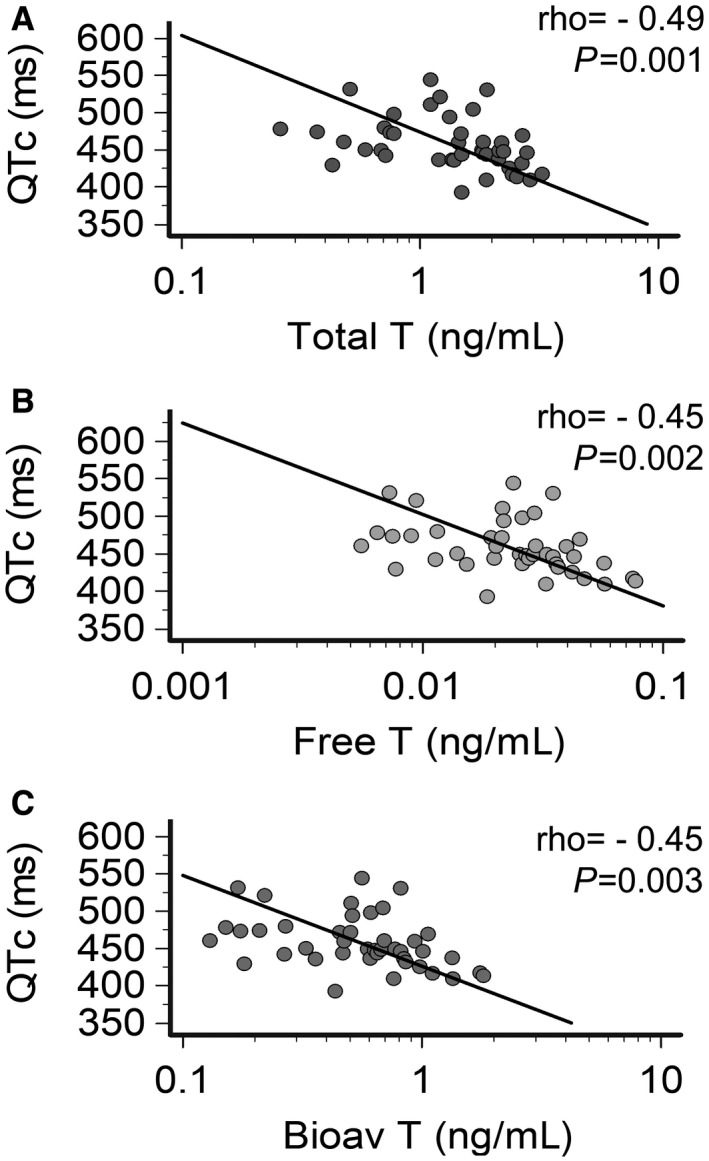
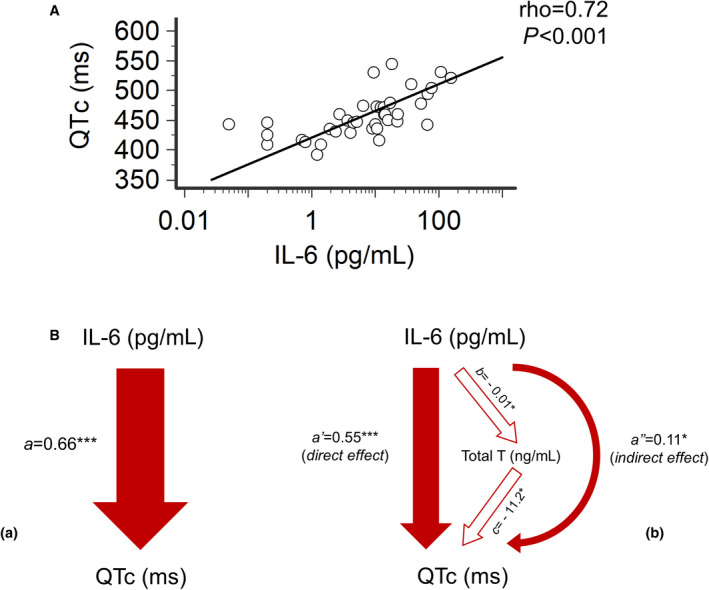
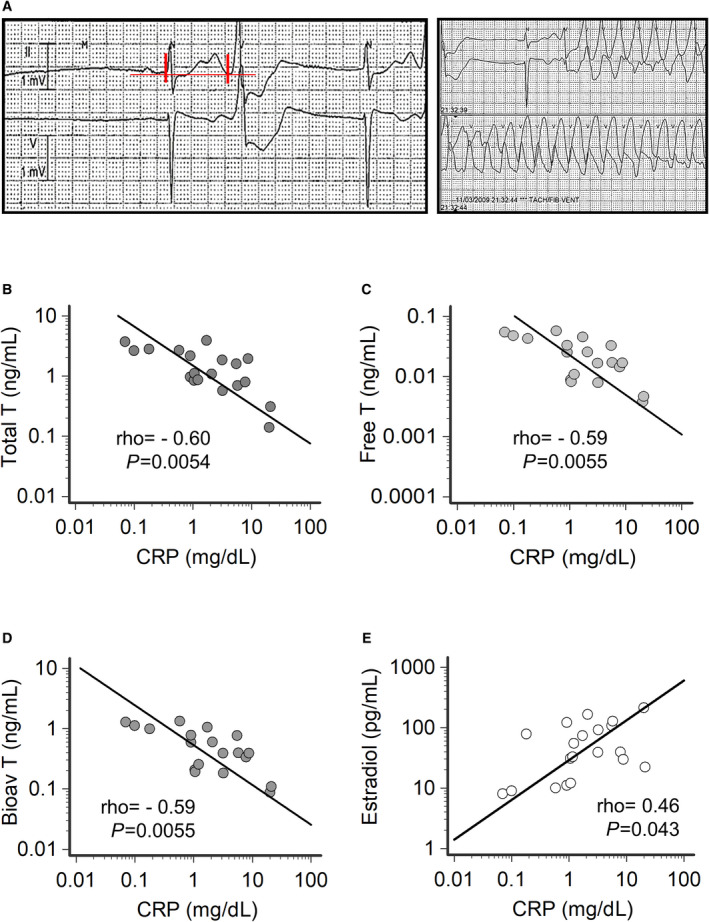
Background Systemic inflammation and male hypogonadism are 2 increasingly recognized "nonconventional" risk factors for long-QT syndrome and torsades de pointes (TdP). Specifically, inflammatory cytokines prolong, while testosterone shortens the heart rate-corrected QT interval (QTc) via direct electrophysiological effects on cardiomyocytes. Moreover, several studies demonstrated important interplays between inflammation and reduced gonad function in men. We hypothesized that, during inflammatory activation in men, testosterone levels decrease and that this enhances TdP risk by contributing to the overall prolonging effect of inflammation on QTc. Methods and Results We investigated (1) the levels of sex hormones and their relationship with inflammatory markers and QTc in male patients with different types of inflammatory diseases, during active phase and recovery; and (2) the association between inflammatory markers and sex hormones in a cohort of male patients who developed extreme QTc prolongation and TdP, consecutively collected over 10 years. In men with active inflammatory diseases, testosterone levels were significantly reduced, but promptly normalized in association with the decrease in C-reactive protein and interleukin-6 levels. Reduction of testosterone levels, which also inversely correlated with 17-β estradiol over time, significantly contributed to inflammation-induced QTc prolongation. In men with TdP, both active systemic inflammation and hypogonadism were frequently present, with significant correlations between C-reactive protein, testosterone, and 17-β estradiol levels; in these patients, increased C-reactive protein and reduced testosterone were associated with a worse short-term outcome of the arrhythmia. Conclusions During systemic inflammatory activation, interleukin-6 elevation is associated with reduced testosterone levels in males, possibly deriving from an enhanced androgen-to-estrogen conversion. While transient, inflammatory hypotestosteronemia is significantly associated with an increased long-QT syndrome/TdP risk in men.
系统性炎症和男性性腺功能减退症是 2 种日益被认可的长 QT 综合征和尖端扭转型室性心动过速(TdP)的“非传统”危险因素。具体而言,炎症细胞因子通过对心肌细胞的直接电生理作用延长心率校正 QT 间期(QTc),而睾酮缩短 QTc。此外,几项研究表明炎症和男性性腺功能减退之间存在重要的相互作用。我们假设,在男性炎症激活期间,睾酮水平下降,这通过增强炎症对 QTc 的整体延长作用来增加 TdP 风险。
我们研究了(1)在患有不同类型炎症性疾病的男性患者中,在活动期和恢复期,性激素水平及其与炎症标志物和 QTc 的关系;(2)在过去 10 年连续收集的发生极度 QTc 延长和 TdP 的男性患者队列中,炎症标志物与性激素之间的关联。在患有活动性炎症性疾病的男性中,睾酮水平显著降低,但与 C 反应蛋白和白细胞介素 6 水平的降低相关,迅速恢复正常。睾酮水平的降低也与 17-β 雌二醇呈负相关,且随时间推移呈下降趋势,这显著导致炎症引起的 QTc 延长。在患有 TdP 的男性中,常同时存在全身炎症和性腺功能减退,C 反应蛋白、睾酮和 17-β 雌二醇水平之间存在显著相关性;在这些患者中,C 反应蛋白升高和睾酮降低与心律失常的短期预后较差相关。
在全身炎症激活期间,白细胞介素 6 升高与男性睾酮水平降低相关,可能源于雄激素向雌激素的转化增强。虽然短暂,但炎症性低睾酮血症与男性长 QT 综合征/TdP 风险增加显著相关。