Van Laethem Johan, Wuyts Stephanie C M, Pierreux Jan, Seyler Lucie, Verschelden Gil, Depondt Thibault, Meuwissen Annelies, Lacor Patrick, Piérard Denis, Allard Sabine D
Department of Internal Medicine, Vrije Universiteit Brussel (VUB), Universitair Ziekenhuis Brussel, UZ Brussel, 1090 Brussels, Belgium.
Hospital Pharmacy, Universitair Ziekenhuis Brussel (UZ Brussel), 1090 Brussels, Belgium.
Antibiotics (Basel). 2021 Dec 6;10(12):1493. doi: 10.3390/antibiotics10121493.
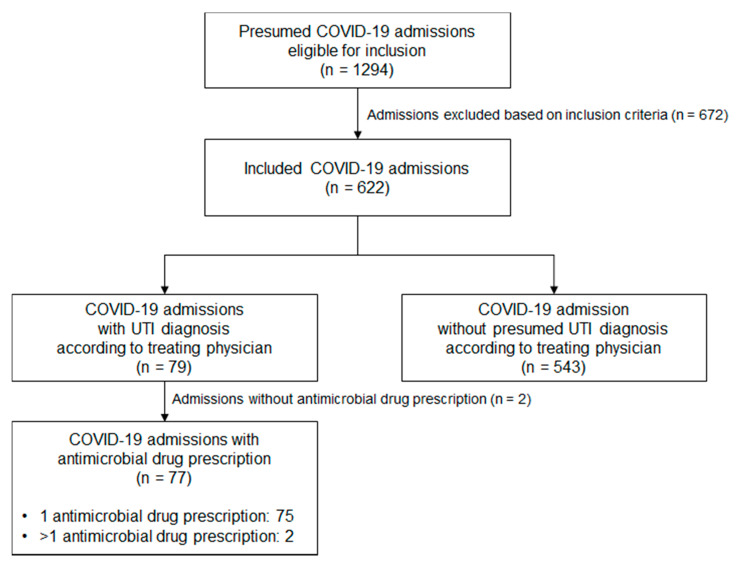
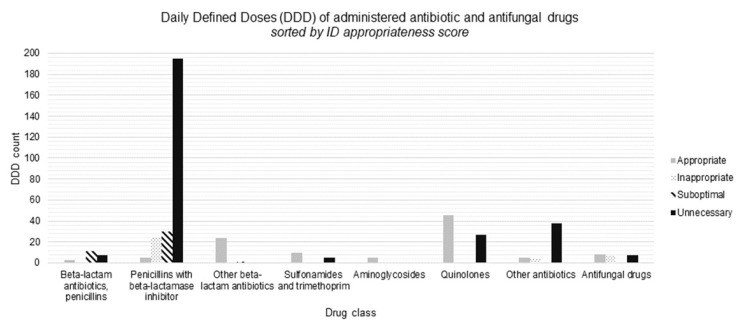
Despite the low rates of bacterial co-/superinfections in COVID-19 patients, antimicrobial drug use has been liberal since the start of the COVID-19 pandemic. Due to the low specificity of markers of bacterial co-/superinfection in the COVID-19 setting, overdiagnosis and antimicrobial overprescription have become widespread. A quantitative and qualitative evaluation of urinary tract infection (UTI) diagnoses and antimicrobial drug prescriptions for UTI diagnoses was performed in patients admitted to the COVID-19 ward of a university hospital between 17 March and 2 November 2020. A team of infectious disease specialists performed an appropriateness evaluation for every diagnosis of UTI and every antimicrobial drug prescription covering a UTI. A driver analysis was performed to identify factors increasing the odds of UTI (over)diagnosis. A total of 622 patients were included. UTI was present in 13% of included admissions, and in 12%, antimicrobials were initiated for a UTI diagnosis (0.71 daily defined doses (DDDs)/admission; 22% were scored as 'appropriate'). An evaluation of UTI diagnoses by ID specialists revealed that of the 79 UTI diagnoses, 61% were classified as probable overdiagnosis related to the COVID-19 hospitalization. The following factors were associated with UTI overdiagnosis: physicians who are unfamiliar working in an internal medicine ward, urinary incontinence, mechanical ventilation and female sex. Antimicrobial stewardship teams should focus on diagnostic stewardship of UTIs, as UTI overdiagnosis seems to be highly prevalent in admitted COVID-19 patients.
尽管新冠病毒病(COVID-19)患者中细菌合并/重叠感染率较低,但自COVID-19大流行开始以来,抗菌药物的使用一直较为随意。由于COVID-19背景下细菌合并/重叠感染标志物的特异性较低,过度诊断和抗菌药物过度处方现象已很普遍。对2020年3月17日至11月2日期间入住某大学医院COVID-19病房的患者进行了尿路感染(UTI)诊断及针对UTI诊断的抗菌药物处方的定量和定性评估。一组传染病专家对每例UTI诊断和每一份涵盖UTI的抗菌药物处方进行了合理性评估。进行驱动因素分析以确定增加UTI(过度)诊断几率的因素。共纳入622例患者。纳入的住院患者中有13%存在UTI,12%因UTI诊断开始使用抗菌药物(0.71日规定剂量(DDD)/住院;22%被评为“合理”)。感染病专家对UTI诊断的评估显示,在79例UTI诊断中,61%被归类为可能与COVID-19住院相关的过度诊断。以下因素与UTI过度诊断相关:不熟悉在内科病房工作的医生、尿失禁、机械通气和女性。抗菌药物管理团队应关注UTI的诊断管理,因为UTI过度诊断在COVID-19住院患者中似乎非常普遍。