Tampe Désirée, Korsten Peter, Bremer Sebastian C B, Winkler Martin S, Tampe Björn
Department of Nephrology and Rheumatology, University Medical Center Göttingen, 37075 Göttingen, Germany.
Department of Gastroenterology, Gastrointestinal Oncology and Endocrinology, University Medical Center Göttingen, 37075 Göttingen, Germany.
Biomedicines. 2021 Dec 5;9(12):1841. doi: 10.3390/biomedicines9121841.
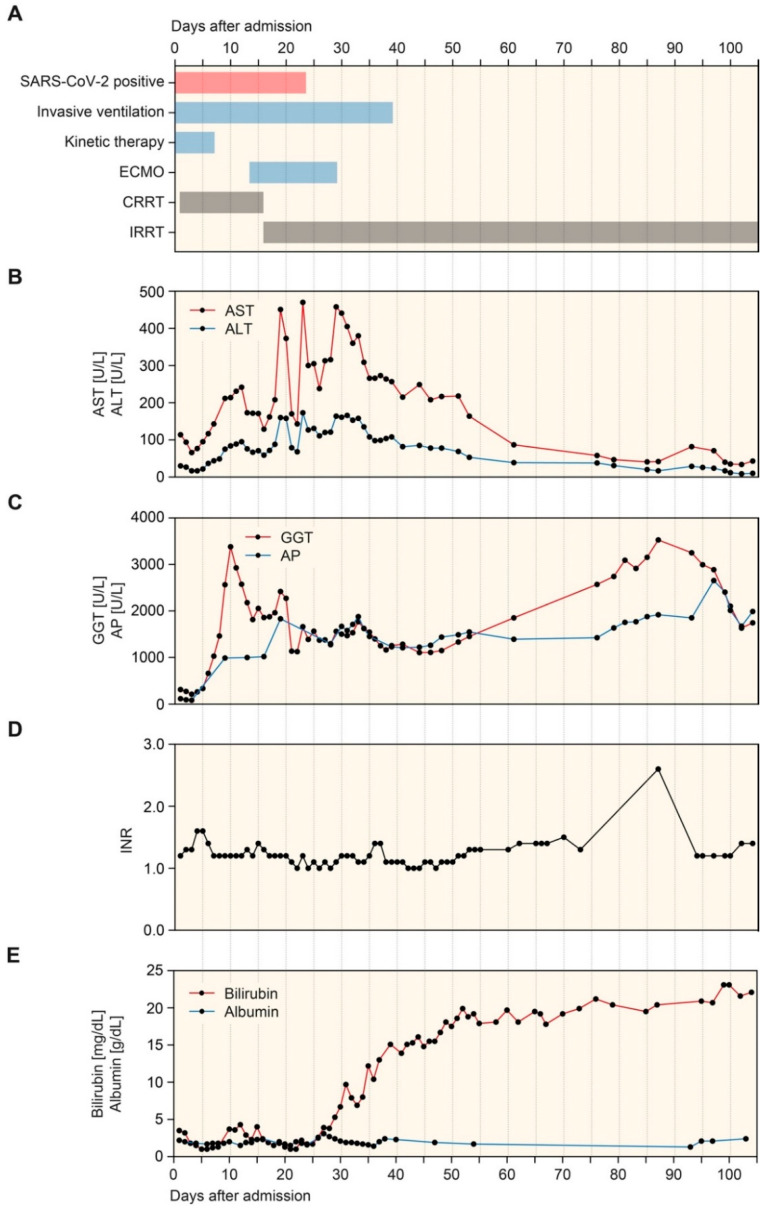
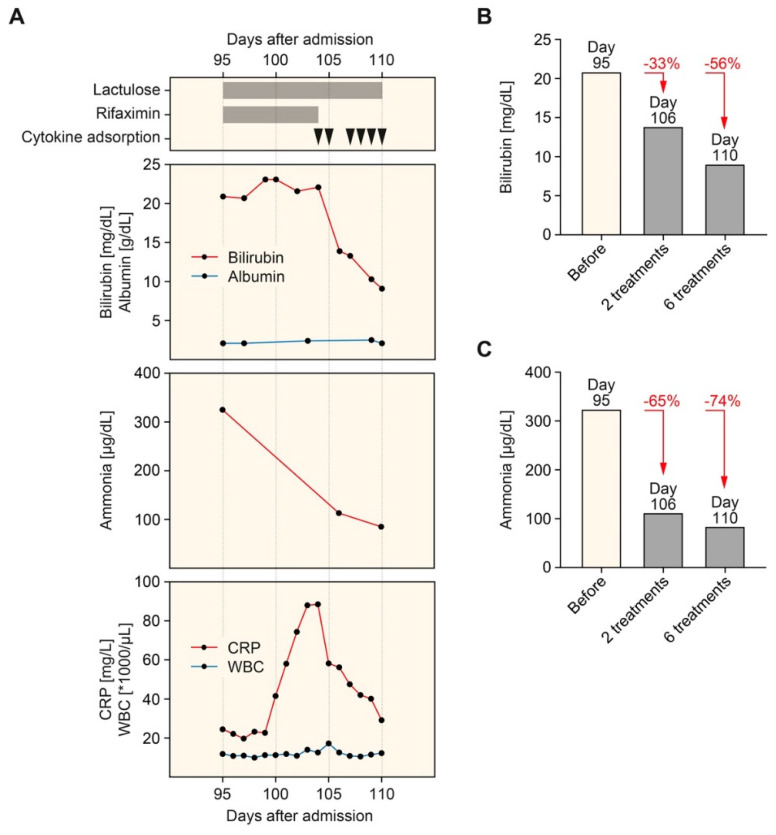
In critically ill patients, liver dysfunction often results in coagulopathy and encephalopathy and is associated with high mortality. Extracorporeal clearance of hepatotoxic metabolites, including bilirubin and ammonia, aims to attenuate further hepatocyte damage and liver injury, resulting in decreased mortality. The efficacy of hemadsorption combined with conventional hemodialysis to eliminate bilirubin and ammonia to support the liver's excretory function in acute liver injury has been described previously. However, the optimal use of liver support systems in chronic liver dysfunction due to secondary sclerosing cholangitis in critically ill patients (SSC-CIP) has not been defined yet. We herein describe the kinetics of successful bilirubin and ammonia elimination by hemadsorption in a patient with SSC-CIP after extracorporeal membrane oxygenation (ECMO) therapy for severe acute respiratory distress syndrome (ARDS) in a patient with coronavirus disease 2019 (COVID-19). During the course of the disease, the patient developed laboratory signs of liver injury during ECMO therapy before clinically detectable jaundice or elevated bilirubin levels. A diagnosis of SSC-CIP was confirmed by endoscopic retrograde cholangiopancreatography (ERCP) based on intraductal filling defects in the intrahepatic bile ducts due to biliary casts. The patient showed stable elevations of bilirubin and ammonia levels thereafter, but presented with progressive nausea, vomiting, weakness, and exhaustion. Based on these laboratory findings, hemadsorption was combined with hemodialysis treatment and successfully eliminated bilirubin and ammonia. Moreover, direct comparison revealed that ammonia is more efficiently eliminated by hemadsorption than bilirubin levels. Clinical symptoms of nausea, vomiting, weakness, and exhaustion improved. In summary, bilirubin and ammonia were successfully eliminated by hemadsorption combined with hemodialysis treatment in SSC-CIP following ECMO therapy and severe COVID-19. This observation is particularly relevant since it has been reported that a considerable subset of critically ill patients with COVID-19 suffer from liver dysfunction associated with high mortality.
在危重症患者中,肝功能障碍常导致凝血功能障碍和肝性脑病,并与高死亡率相关。体外清除肝毒性代谢产物,包括胆红素和氨,旨在减轻进一步的肝细胞损伤和肝损伤,从而降低死亡率。血液吸附联合传统血液透析清除胆红素和氨以支持急性肝损伤中肝脏排泄功能的疗效此前已有描述。然而,对于危重症患者继发硬化性胆管炎导致的慢性肝功能障碍(SSC-CIP)中肝脏支持系统的最佳应用尚未明确。我们在此描述了一名2019冠状病毒病(COVID-19)患者在接受体外膜肺氧合(ECMO)治疗严重急性呼吸窘迫综合征(ARDS)后,通过血液吸附成功清除胆红素和氨的动力学情况。在疾病过程中,患者在ECMO治疗期间出现了肝损伤的实验室指标,此时临床上尚未检测到黄疸或胆红素水平升高。基于肝内胆管因胆管铸型导致的导管内充盈缺损,经内镜逆行胰胆管造影(ERCP)确诊为SSC-CIP。此后患者胆红素和氨水平持续稳定升高,但出现了进行性恶心、呕吐、虚弱和疲惫。基于这些实验室检查结果,血液吸附联合血液透析治疗,成功清除了胆红素和氨。此外,直接比较显示,血液吸附清除氨比清除胆红素水平更有效。恶心、呕吐、虚弱和疲惫的临床症状得到改善。总之,在ECMO治疗和重症COVID-19后的SSC-CIP患者中,血液吸附联合血液透析治疗成功清除了胆红素和氨。这一观察结果尤为重要,因为据报道,相当一部分重症COVID-19患者存在与高死亡率相关的肝功能障碍。