Bongiovanni Filippo, Grieco Domenico Luca, Anzellotti Gian Marco, Menga Luca Salvatore, Michi Teresa, Cesarano Melania, Raggi Valeria, De Bartolomeo Cecilia, Mura Benedetta, Mercurio Giovanna, D'Arrigo Sonia, Bello Giuseppe, Maviglia Riccardo, Pennisi Mariano Alberto, Antonelli Massimo
Department of Anesthesiology and Intensive Care Medicine, Catholic University of The Sacred Heart, Rome, Italy.
Anesthesia, Emergency and Intensive Care Medicine, Fondazione Policlinico Universitario A. Gemelli IRCCS, L.Go F. Vito, 00168, Rome, Italy.
Ann Intensive Care. 2021 Dec 24;11(1):184. doi: 10.1186/s13613-021-00972-9.
There is growing interest towards the use of helmet noninvasive ventilation (NIV) for the management of acute hypoxemic respiratory failure. Gas conditioning through heat and moisture exchangers (HME) or heated humidifiers (HHs) is needed during facemask NIV to provide a minimum level of humidity in the inspired gas (15 mg HO/L). The optimal gas conditioning strategy during helmet NIV remains to be established.
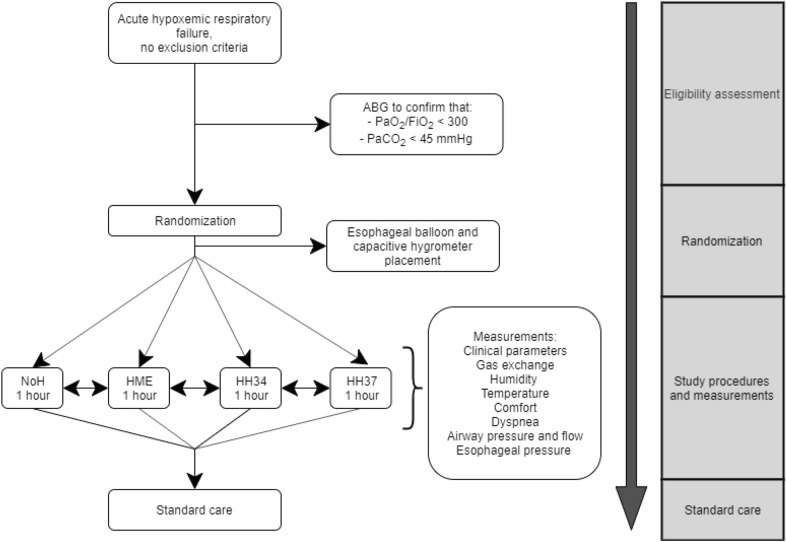
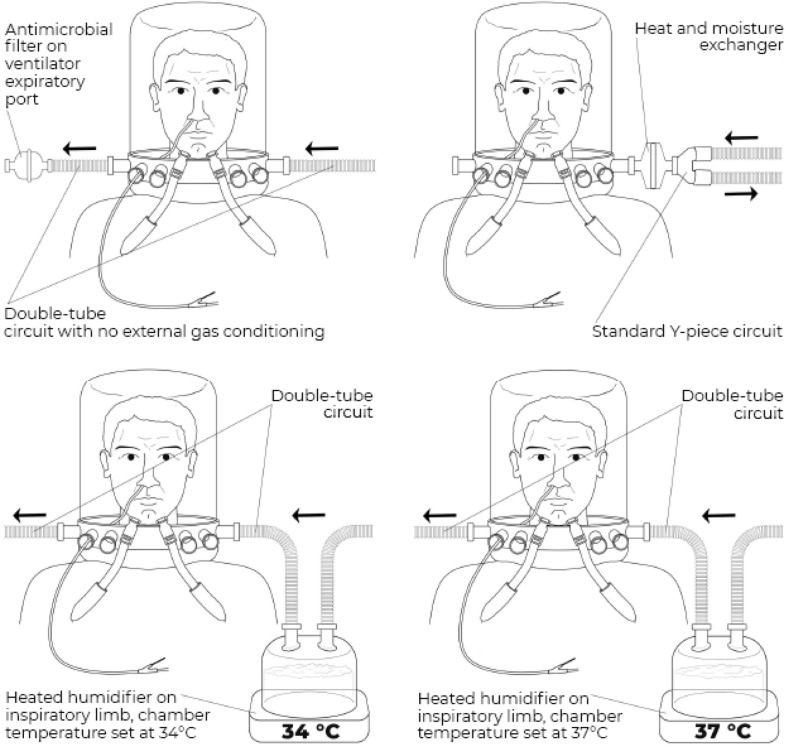
Twenty patients with acute hypoxemic respiratory failure (PaO/FiO < 300 mmHg) underwent consecutive 1-h periods of helmet NIV (PEEP 12 cmHO, pressure support 12 cmHO) with four humidification settings, applied in a random order: double-tube circuit with HHs and temperature set at 34 °C (HH34) and 37 °C (HH37); Y-piece circuit with HME; double-tube circuit with no humidification (NoH). Temperature and humidity of inhaled gas were measured through a capacitive hygrometer. Arterial blood gases, discomfort and dyspnea through visual analog scales (VAS), esophageal pressure swings (ΔP) and simplified pressure-time product (PTP), dynamic transpulmonary driving pressure (ΔP) and asynchrony index were measured in each step.
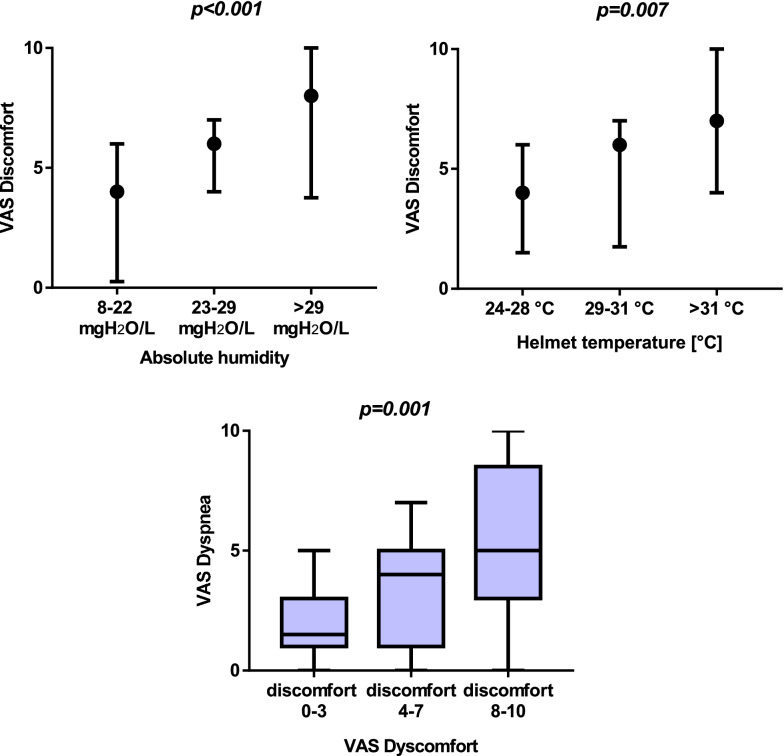
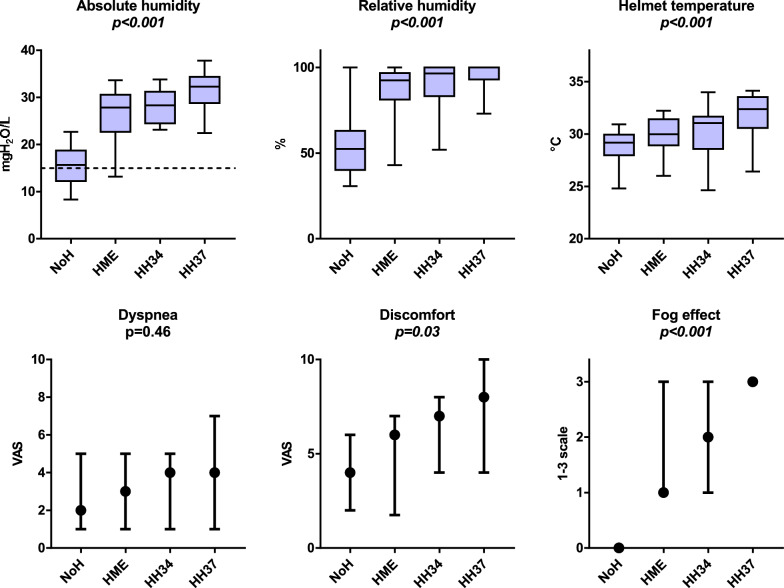
Median [IqR] absolute humidity, temperature and VAS discomfort were significantly lower during NoH vs. HME, HH34 and HH37: absolute humidity (mgHO/L) 16 [12-19] vs. 28 [23-31] vs. 28 [24-31] vs. 33 [29-38], p < 0.001; temperature (°C) 29 [28-30] vs. 30 [29-31] vs. 31 [29-32] vs 32. [31-33], p < 0.001; VAS discomfort 4 [2-6] vs. 6 [2-7] vs. 7 [4-8] vs. 8 [4-10], p = 0.03. VAS discomfort increased with higher absolute humidity (p < 0.01) and temperature (p = 0.007). Higher VAS discomfort was associated with increased VAS dyspnea (p = 0.001). Arterial blood gases, respiratory rate, ΔP, PTP and ΔP were similar in all conditions. Overall asynchrony index was similar in all steps, but autotriggering rate was lower during NoH and HME (p = 0.03).
During 1-h sessions of helmet NIV in patients with hypoxemic respiratory failure, a double-tube circuit with no humidification allowed adequate conditioning of inspired gas, optimized comfort and improved patient-ventilator interaction. Use of HHs or HME in this setting resulted in increased discomfort due to excessive heat and humidity in the interface, which was associated with more intense dyspnea. Trail Registration Registered on clinicaltrials.gov (NCT02875379) on August 23rd, 2016.
头盔无创通气(NIV)用于急性低氧性呼吸衰竭的治疗越来越受到关注。面罩无创通气期间需要通过热湿交换器(HME)或加热湿化器(HH)进行气体调节,以在吸入气体中提供最低湿度水平(15mg HO/L)。头盔无创通气期间的最佳气体调节策略仍有待确定。
20例急性低氧性呼吸衰竭患者(PaO/FiO<300mmHg)接受连续1小时的头盔无创通气(呼气末正压12cmHO,压力支持12cmHO),采用四种湿化设置,随机顺序应用:双管回路加加热湿化器且温度设置为34°C(HH34)和37°C(HH37);Y型管回路加HME;无湿化的双管回路(NoH)。通过电容式湿度计测量吸入气体的温度和湿度。在每个步骤中测量动脉血气、通过视觉模拟量表(VAS)评估的不适和呼吸困难、食管压力波动(ΔP)和简化压力-时间乘积(PTP)、动态跨肺驱动压力(ΔP)和不同步指数。
与HME、HH34和HH37相比,NoH期间的中位[IqR]绝对湿度、温度和VAS不适显著更低:绝对湿度(mgHO/L)16[12 - 19]对比28[23 - 31]对比28[24 - 31]对比33[29 - 38],p<0.001;温度(°C)29[28 - 30]对比30[29 - 31]对比31[29 - 32]对比32[31 - 33],p<0.001;VAS不适4[2 - 6]对比6[2 - 7]对比7[4 - 8]对比8[4 - 10],p = 0.03。VAS不适随绝对湿度升高(p<0.01)和温度升高(p = 0.007)而增加。更高的VAS不适与VAS呼吸困难增加相关(p = 0.001)。所有条件下动脉血气、呼吸频率、ΔP、PTP和ΔP相似。所有步骤的总体不同步指数相似,但NoH和HME期间的自动触发率更低(p = 0.03)。
在低氧性呼吸衰竭患者进行1小时头盔无创通气期间,无湿化的双管回路可实现对吸入气体的充分调节,优化舒适度并改善患者与呼吸机的相互作用。在此设置下使用加热湿化器或HME会因界面处过热和过湿而导致不适增加,这与更强烈的呼吸困难相关。试验注册于2016年8月23日在clinicaltrials.gov上注册(NCT02875379)。