Di Nardo Matteo, Boldrini Francesca, Broccati Francesca, Cancani Federica, Satta Tiziana, Stoppa Francesca, Genuini Leonardo, Zampini Giorgio, Perdichizzi Salvatore, Bottari Gabriella, Fischer Maximilian, Gawronski Orsola, Bonetti Annamaria, Piermarini Irene, Recchiuti Veronica, Leone Paola, Rossi Angela, Tabarini Paola, Biasucci Daniele, Villani Alberto, Raponi Massimiliano, Cecchetti Corrado, Choong Karen
PICU, Children's Hospital Bambino Gesù, Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS), Rome, Italy.
Unit of Clinical Psychology, Department of Neurological Sciences, Children's Hospital Bambino Gesù, Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS), Rome, Italy.
Front Pediatr. 2021 Dec 8;9:788997. doi: 10.3389/fped.2021.788997. eCollection 2021.
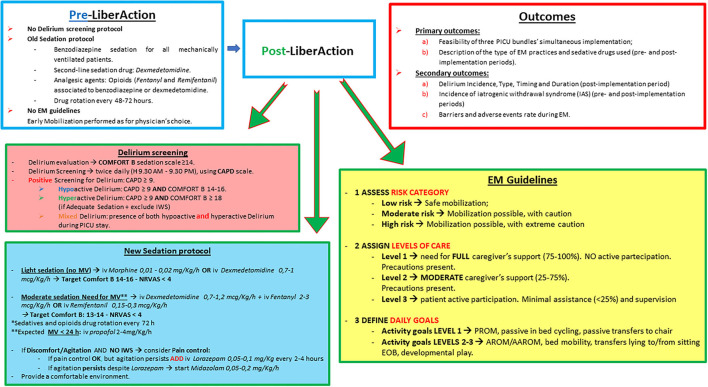
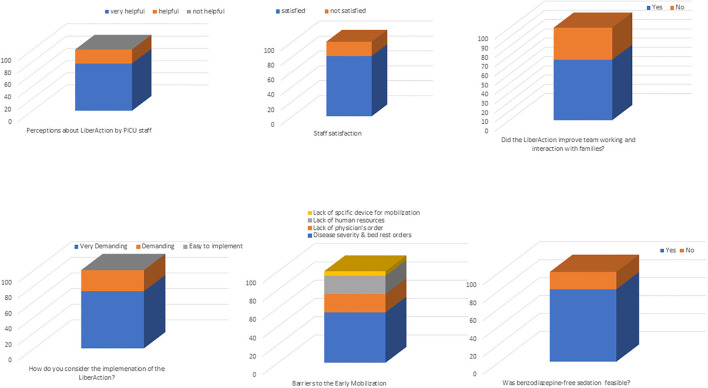
Delirium, bed immobilization, and heavy sedation are among the major contributors of pediatric post-intensive care syndrome. Recently, the Society of Critical Care Medicine has proposed the implementation of daily interventions to minimize the incidence of these morbidities and optimize children functional outcomes and quality of life. Unfortunately, these interventions require important clinical and economical efforts which prevent their use in many pediatric intensive care units (PICU). First, to evaluate the feasibility and safety of a PICU bundle implementation prioritizing delirium screening and treatment, early mobilization (<72 h from PICU admission) and benzodiazepine-limited sedation in a human resource-limited PICU. Second, to evaluate the incidence of delirium and describe the early mobilization practices and sedative drugs used during the pre- and post-implementation periods. Third, to describe the barriers and adverse events encountered during early mobilization. This observational study was structured in a pre- (15th November 2019-30th June 2020) and post-implementation period (1st July 2020-31st December 2020). All patients admitted in PICU for more than 72 h during the pre and post-implementation period were included in the study. Patients were excluded if early mobilization was contraindicated. During the pre-implementation period, a rehabilitation program including delirium screening and treatment, early mobilization and benzodiazepine-sparing sedation guidelines was developed and all PICU staff trained. During the post-implementation period, delirium screening with the Connell Assessment of Pediatric Delirium scale was implemented at bedside. Early mobilization was performed using a structured tiered protocol and a new sedation protocol, limiting the use of benzodiazepine, was adopted. Two hundred and twenty-five children were enrolled in the study, 137 in the pre-implementation period and 88 in the post-implementation period. Adherence to delirium screening, benzodiazepine-limited sedation and early mobilization was 90.9, 81.1, and 70.4%, respectively. Incidence of delirium was 23% in the post-implementation period. The median cumulative dose of benzodiazepines corrected for the total number of sedation days (mg/kg/sedation days) was significantly lower in the post-implementation period compared with the pre-implementation period: [0.83 (IQR: 0.53-1.31) vs. 0.74 (IQR: 0.55-1.16), = 0.0001]. The median cumulative doses of fentanyl, remifentanil, and morphine corrected for the total number of sedation days were lower in the post-implementation period, but these differences were not significant. The median number of mobilizations per patient and the duration of each mobilization significantly increased in the post-implementation period [3.00 (IQR: 2.0-4.0) vs. 7.00 (IQR: 3.0-12.0); = 0.004 and 4 min (IQR: 3.50-4.50) vs. 5.50 min (IQR: 5.25-6.5); < 0.0001, respectively]. Barriers to early mobilization were: disease severity and bed rest orders (55%), lack of physicians' order (20%), lack of human resources (20%), and lack of adequate devices for patient mobilization (5%). No adverse events related to early mobilization were reported in both periods. Duration of mechanical ventilation and PICU length of stay was significantly lower in the post-implementation period as well as the occurrence of iatrogenic withdrawal syndrome. This study showed that the implementation of a PICU liberation bundle prioritizing delirium screening and treatment, benzodiazepine-limited sedation and early mobilization was feasible and safe even in a human resource-limited PICU. Further pediatric studies are needed to evaluate the clinical impact of delirium, benzodiazepine-limited sedation and early mobilization protocols on patients' long-term functional outcomes and on hospital finances.
谵妄、卧床制动和深度镇静是小儿重症监护后综合征的主要促成因素。最近,危重症医学会提议实施日常干预措施,以尽量减少这些病症的发生率,并优化儿童的功能结局和生活质量。不幸的是,这些干预措施需要大量的临床和经济投入,这使得它们在许多儿科重症监护病房(PICU)中无法得到应用。第一,评估在人力资源有限的PICU中实施以谵妄筛查和治疗、早期活动(PICU入院后<72小时)和苯二氮䓬类药物限制镇静为重点的PICU集束化治疗的可行性和安全性。第二,评估谵妄的发生率,并描述实施前后期间使用的早期活动措施和镇静药物。第三,描述早期活动期间遇到的障碍和不良事件。这项观察性研究分为实施前(2019年11月15日至2020年6月30日)和实施后(2020年7月1日至2020年12月31日)两个阶段。实施前后期间入住PICU超过72小时的所有患者均纳入研究。如果早期活动存在禁忌证,则将患者排除。在实施前阶段,制定了包括谵妄筛查和治疗、早期活动以及苯二氮䓬类药物节省镇静指南的康复计划,并对所有PICU工作人员进行了培训。在实施后阶段,在床边使用康奈尔小儿谵妄评估量表进行谵妄筛查。采用结构化分层方案进行早期活动,并采用新的镇静方案,限制苯二氮䓬类药物的使用。共有225名儿童参与研究,实施前阶段137名,实施后阶段88名。谵妄筛查、苯二氮䓬类药物限制镇静和早期活动的依从率分别为90.9%、81.1%和70.4%。实施后阶段谵妄的发生率为23%。与实施前阶段相比,实施后阶段按镇静天数校正的苯二氮䓬类药物累计中位剂量显著降低:[0.83(四分位间距:0.53 - 1.31)对0.74(四分位间距:0.55 - 1.16),P = 0.0001]。按镇静天数校正的芬太尼、瑞芬太尼和吗啡的累计中位剂量在实施后阶段较低,但这些差异不显著。实施后阶段每位患者的活动次数中位数和每次活动的持续时间显著增加[3.00(四分位间距:2.0 - 4.0)对7.00(四分位间距:3.0 - 12.0);P = 0.004和4分钟(四分位间距:3.50 - 4.50)对5.50分钟(四分位间距:5.25 - 6.5);P均<0.0001]。早期活动的障碍包括:疾病严重程度和卧床医嘱(55%)、缺乏医生医嘱(20%)、缺乏人力资源(20%)以及缺乏适合患者活动的设备(5%)。两个阶段均未报告与早期活动相关的不良事件。实施后阶段机械通气时间和PICU住院时间显著缩短,医源性戒断综合征的发生率也显著降低。这项研究表明,即使在人力资源有限的PICU中,实施以谵妄筛查和治疗、苯二氮䓬类药物限制镇静和早期活动为重点的PICU解放集束化治疗也是可行和安全的。需要进一步开展儿科研究,以评估谵妄、苯二氮䓬类药物限制镇静和早期活动方案对患者长期功能结局和医院财务状况的临床影响。