Division of Gastroenterology, University of California San Diego, La Jolla, CA, USA.
IBD Unit, Fondazione Policlinico Universitario A. Gemelli IRCCS, Università Cattolica del Sacro Cuore, Rome, Italy.
Inflamm Bowel Dis. 2022 Sep 1;28(9):1338-1347. doi: 10.1093/ibd/izab278.
Tofacitinib is an oral, small molecule JAK inhibitor for the treatment of ulcerative colitis. We evaluate baseline characteristics as predictors of sustained response and remission in patients with ulcerative colitis receiving tofacitinib maintenance therapy.
Patients with clinical response following OCTAVE Induction 1 and 2 entered OCTAVE Sustain and were rerandomized to receive tofacitinib 5 or 10 mg twice daily or placebo. Baseline characteristics were stratified by week 52 efficacy endpoints (remission, sustained remission, clinical response, sustained clinical response). Associations between baseline characteristics and efficacy endpoints were evaluated using logistic regression analyses.
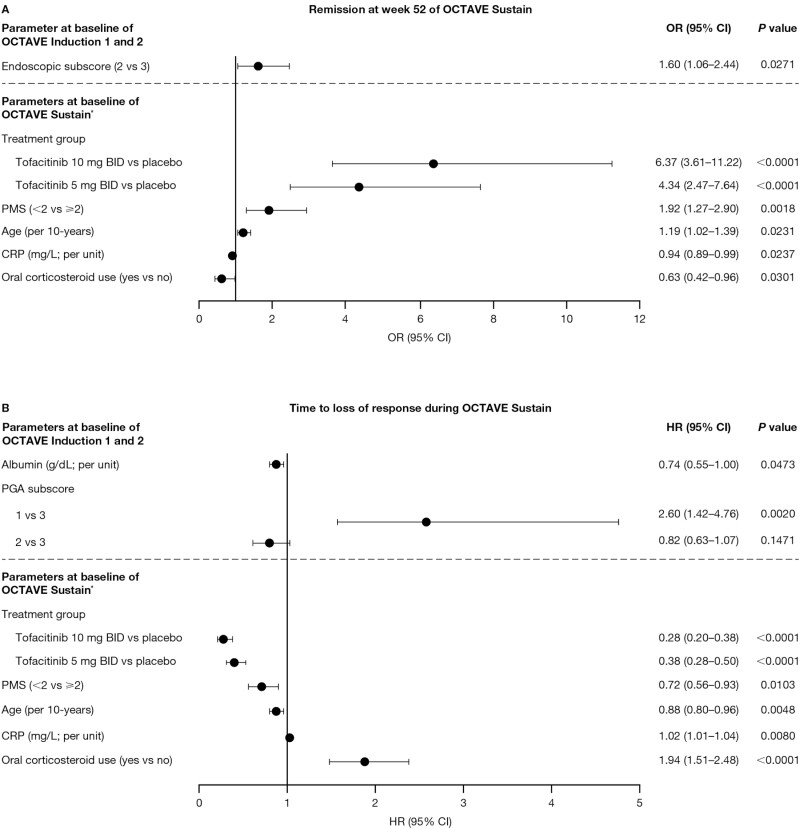
Overall, 170 of 487 (34.9%) patients were in remission at week 52. In multivariable modeling, endoscopic subscore at baseline of OCTAVE Induction 1 and 2 (2 vs 3; odds ratio [OR], 1.60; 95% confidence interval [CI], 1.06-2.44]), partial Mayo score (<2 vs ≥2; OR, 1.92; 95% CI, 1.27-2.90), and age (per 10-years; OR, 1.19; 95% CI, 1.02-1.39) at baseline of OCTAVE Sustain (following 8 weeks' tofacitinib induction therapy) were associated with higher odds of remission at week 52. Oral corticosteroid use (OR, 0.63; 95% CI, 0.42-0.96) and C-reactive protein (per unit; OR, 0.94; 95% CI, 0.89-0.99) at baseline of OCTAVE Sustain were associated with reduced likelihood of remission at week 52. In general, opposite associations were observed for time to loss of response.
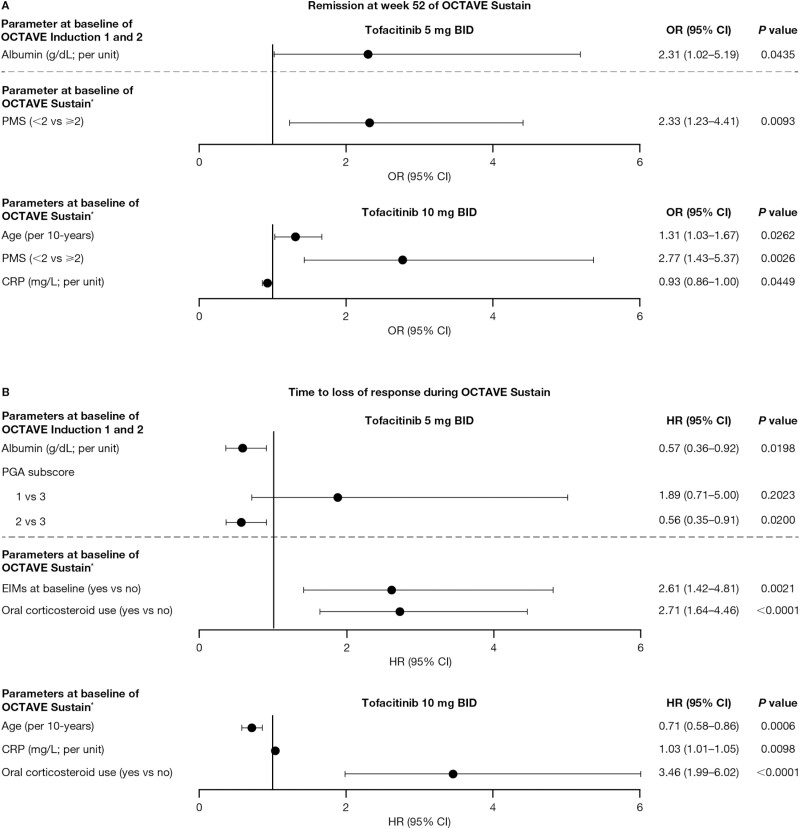
Patients with greater clinical improvement after 8 weeks of tofacitinib induction therapy are more likely to maintain response or remission with tofacitinib regardless of dose received during maintenance, highlighting the importance of a robust response to induction therapy.
托法替布是一种用于治疗溃疡性结肠炎的口服小分子 JAK 抑制剂。我们评估了基线特征,以预测接受托法替布维持治疗的溃疡性结肠炎患者的持续缓解和缓解。
在 OCTAVE 诱导 1 和 2 中获得临床缓解的患者进入 OCTAVE 维持期,并重新随机分配接受托法替布 5 或 10mg 每日两次或安慰剂。根据第 52 周的疗效终点(缓解、持续缓解、临床缓解、持续临床缓解)对基线特征进行分层。使用逻辑回归分析评估基线特征与疗效终点之间的关联。
总体而言,487 例患者中有 170 例(34.9%)在第 52 周时缓解。在多变量模型中,OCTAVE 诱导 1 和 2 的基线内镜下评分(2 分与 3 分;比值比 [OR],1.60;95%置信区间 [CI],1.06-2.44)、部分 Mayo 评分(<2 分与≥2 分;OR,1.92;95%CI,1.27-2.90)和年龄(每 10 岁;OR,1.19;95%CI,1.02-1.39)与第 52 周的缓解几率较高相关。OCTAVE 维持期(托法替布诱导治疗 8 周后)时的口服皮质类固醇使用(OR,0.63;95%CI,0.42-0.96)和 C 反应蛋白(每单位;OR,0.94;95%CI,0.89-0.99)与第 52 周时缓解的可能性降低相关。一般来说,对于失去反应的时间,观察到相反的关联。
接受托法替布诱导治疗 8 周后临床改善更大的患者,无论维持治疗期间接受何种剂量的托法替布,更有可能维持缓解或缓解,这凸显了诱导治疗获得稳健反应的重要性。