British Heart Foundation Cardiovascular Research Centre, University of Glasgow, Glasgow, UK.
Division of Health Sciences, Hangzhou Normal University, Hangzhou, China.
Eur J Heart Fail. 2022 Mar;24(3):551-561. doi: 10.1002/ejhf.2419. Epub 2022 Jan 19.
Sudden death is a leading cause of mortality in heart failure with reduced ejection fraction (HFrEF). In PARADIGM-HF, sacubitril/valsartan reduced the incidence of sudden death. The purpose of this post hoc study was to analyse the effect of sacubitril/valsartan, compared to enalapril, on the incidence of ventricular arrhythmias.
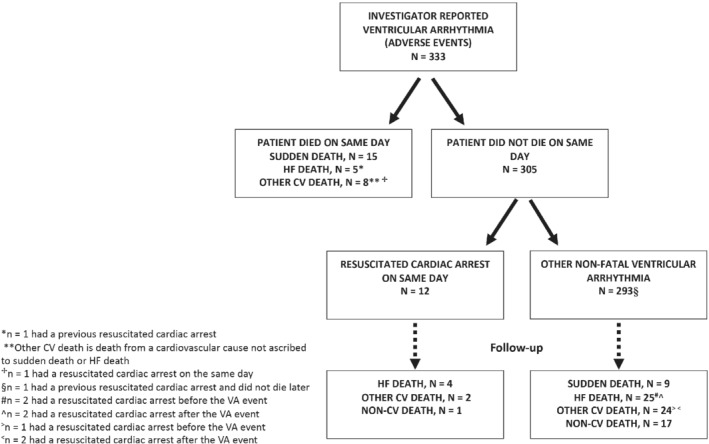
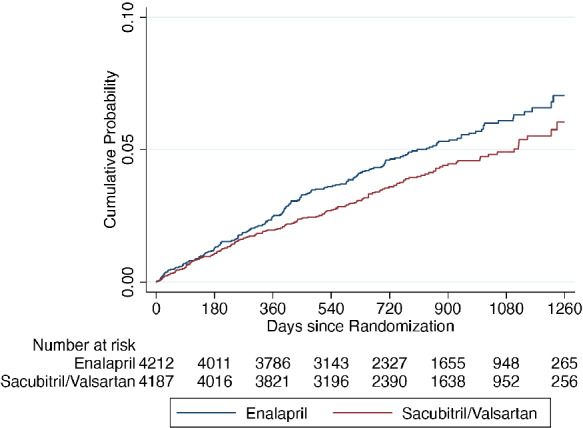
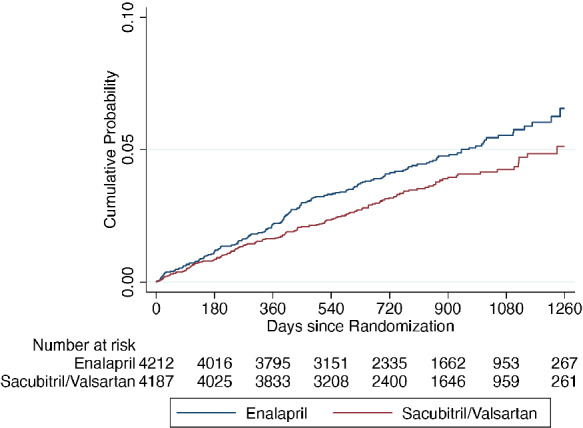
Adverse event reports related to ventricular arrhythmias were examined in PARADIGM-HF. The effect of randomized treatment on two arrhythmia outcomes was analysed: ventricular arrhythmias and the composite of a ventricular arrhythmia, implantable cardioverter defibrillator (ICD) shock or resuscitated cardiac arrest. The risk of death related to a ventricular arrhythmia was examined in time-updated models. The interaction between heart failure aetiology, or baseline ICD/cardiac resynchronization therapy-defibrillator (CRT-D) use, and the effect of sacubitril/valsartan was analysed. Of the 8399 participants, 333 (4.0%) reported a ventricular arrhythmia and 372 (4.4%) the composite arrhythmia outcome. Ventricular arrhythmias were associated with higher mortality. Compared with enalapril, sacubitril/valsartan reduced the risk of a ventricular arrhythmia (hazard ratio [HR] 0.76, 95% confidence interval [CI] 0.62-0.95; p = 0.015) and the composite arrhythmia outcome (HR 0.79, 95% CI 0.65-0.97; p = 0.025). The treatment effect was maintained after adjustment and accounting for the competing risk of death. Baseline ICD/CRT-D use did not modify the effect of sacubitril/valsartan, but aetiology did: HR in patients with an ischaemic aetiology 0.93 (95% CI 0.71-1.21) versus 0.53 (95% CI 0.37-0.78) in those without an ischaemic aetiology (p for interaction = 0.020).
Sacubitril/valsartan reduced the incidence of investigator-reported ventricular arrhythmias in patients with HFrEF. This effect may have been greater in patients with a non-ischaemic aetiology.
心力衰竭伴射血分数降低(HFrEF)患者的主要死亡原因是猝死。在 PARADIGM-HF 研究中,沙库巴曲缬沙坦降低了猝死的发生率。本事后分析旨在分析与依那普利相比,沙库巴曲缬沙坦对室性心律失常发生率的影响。
在 PARADIGM-HF 研究中,对与室性心律失常相关的不良事件报告进行了检查。分析了随机治疗对两种心律失常结局的影响:室性心律失常和室性心律失常、植入式心脏复律除颤器(ICD)电击或复苏性心脏骤停的复合终点。在时间更新模型中检查了与室性心律失常相关的死亡风险。分析了心力衰竭病因或基线 ICD/心脏再同步治疗除颤器(CRT-D)使用与沙库巴曲缬沙坦作用之间的相互作用。在 8399 名参与者中,333 名(4.0%)报告了室性心律失常,372 名(4.4%)报告了复合心律失常结局。室性心律失常与死亡率升高相关。与依那普利相比,沙库巴曲缬沙坦降低了室性心律失常的风险(风险比 [HR] 0.76,95%置信区间 [CI] 0.62-0.95;p=0.015)和复合心律失常结局的风险(HR 0.79,95% CI 0.65-0.97;p=0.025)。调整后和考虑死亡竞争风险后,治疗效果仍然存在。基线 ICD/CRT-D 的使用并未改变沙库巴曲缬沙坦的作用,但病因学确实有影响:缺血性病因患者的 HR 为 0.93(95%CI 0.71-1.21),而非缺血性病因患者的 HR 为 0.53(95%CI 0.37-0.78)(p 交互=0.020)。
沙库巴曲缬沙坦降低了 HFrEF 患者报告的室性心律失常发生率。这种效果在非缺血性病因患者中可能更大。