Zheng Yue, Zhang Haiyin, Fan Qing
East China University of Science and Technology, Shanghai, China.
Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine, Shanghai, China.
Gen Psychiatr. 2021 Dec 10;34(6):e100576. doi: 10.1136/gpsych-2021-100576. eCollection 2021.
Developing accurate identification methods for individuals with suicide attempts and providing them with follow-up care and supports can be a vital component of all comprehensive suicide prevention strategies. However, because of the difficulties concerning one's intentions behind injurious behaviour, identifying suicide attempts is a challenge for families and clinicians.
The aim of this study was to investigate the differences between family report and clinical assessment for suicide attempts in the emergency department (ED).
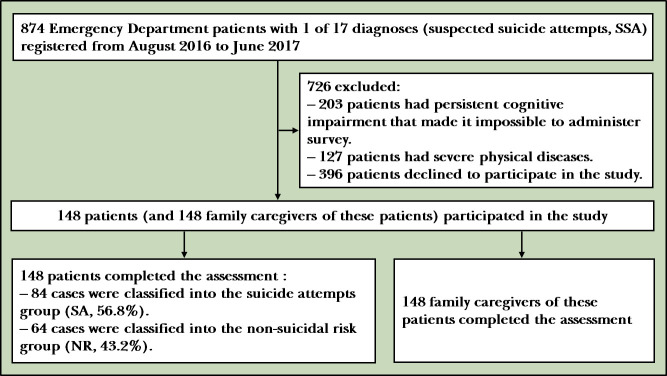
A total of 148 patients with suspected suicide attempts (SSAs) and 148 family caregivers in the ED were enrolled. The suicide risk module of the Chinese version of the MINI International Neuropsychiatric Interview and the self-report measure were used to assess those with SSA's suicidal behaviours. The Family Adaptability and Cohesion Evaluation Scales and semi-structured interviews were used to investigate the characteristics of suicide risk and demographics of patients with SSA, as well as the rate and influencing factors of omitted suicide attempts reported by family caregivers.
The underreporting rate for family reported suicide attempts in the ED was 69.0%. The suicide attempts group indicated lower mean scores on perceptions of family resources, adaptability and cohesion. Patients' suicide risk rating (OR =-1.81, 95% CI: -3.87 to -0.33, p=0.036), family satisfaction (OR =-1.11, 95% CI: -2.29 to -0.06, p=0.048), and caregiver's age (OR =-1.68, 95% CI: -3.10 to -0.48, p=0.010) might be associated with underreporting by families. If patients committed suicide attempts through a falling injury or medication overdose, their families may have misreported the suicide attempt.
The discordance of suicide attempt records between family report and clinical assessment reveals the limitations of family self-reports when identifying suicide attempts. Interviews and observations, together with information from certain diagnoses, should be combined to accurately identify suicide attempters in the ED.
开发针对有自杀未遂行为个体的准确识别方法,并为他们提供后续护理和支持,可能是所有综合自杀预防策略的重要组成部分。然而,由于伤害行为背后个人意图的复杂性,识别自杀未遂行为对家庭和临床医生来说是一项挑战。
本研究旨在调查急诊科(ED)中家庭报告与自杀未遂临床评估之间的差异。
共纳入148例急诊科疑似自杀未遂(SSA)患者及148名家庭照顾者。使用中文版迷你国际神经精神访谈的自杀风险模块和自我报告量表评估SSA患者的自杀行为。采用家庭适应性和凝聚性评估量表及半结构式访谈,调查SSA患者的自杀风险特征、人口统计学特征,以及家庭照顾者报告的漏报自杀未遂行为的发生率和影响因素。
急诊科家庭报告的自杀未遂漏报率为69.0%。自杀未遂组在家庭资源、适应性和凝聚性认知方面的平均得分较低。患者的自杀风险评级(OR = -1.81,95%CI:-3.87至-0.33,p = 0.036)、家庭满意度(OR = -1.11,95%CI:-2.29至-0.06,p = 0.048)和照顾者年龄(OR = -1.68,95%CI:-3.10至-0.48,p = 0.010)可能与家庭漏报有关。如果患者通过坠伤或药物过量实施自杀未遂,其家庭可能会误报自杀未遂行为。
家庭报告与临床评估之间自杀未遂记录的不一致揭示了家庭自我报告在识别自杀未遂行为时的局限性。应结合访谈、观察以及某些诊断信息,以准确识别急诊科的自杀未遂者。