Department of Urology and Andrology, Shanghai Institute of Andrology, Renji Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200001, China.
Department of Urology, Yantai Affiliated Hospital of Binzhou Medical University, Yantai 264100, China.
Asian J Androl. 2022 Sep-Oct;24(5):473-477. doi: 10.4103/aja202189.
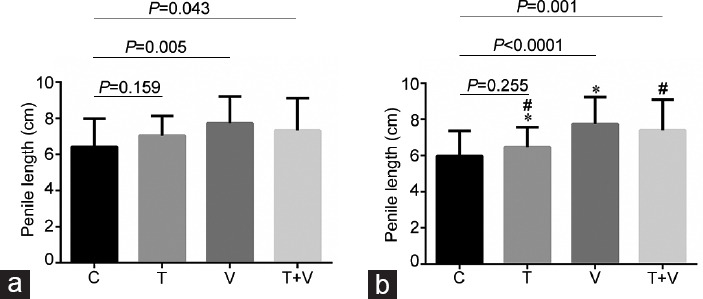
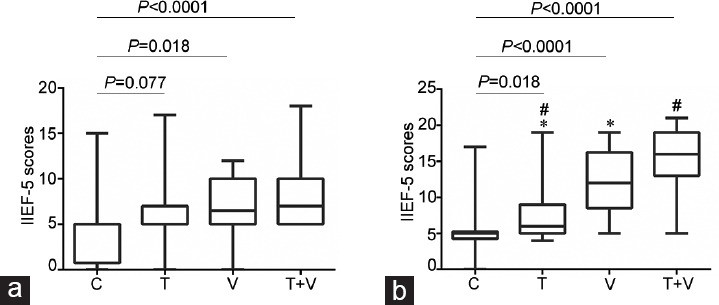
Cavernous nerve injury is an important cause of erectile dysfunction (ED). Although protective nerve technology has been widely used in nerve-sparing radical prostatectomy (nsRP), the incidence of ED is still very high after surgery. The purpose of our study was to evaluate erectile function (EF) and penile length in the non-erectile state (PLNES) following scheduled phosphodiesterase 5 inhibitor (PDE5i), vacuum erectile device (VED) treatment, and combination therapy after nsRP. One hundred patients with localized prostate cancer and normal EF were randomized to scheduled PDE5i group, VED treatment group, a combined treatment group, and the control group without any intervention. The International Index of Erectile Function-5 (IIEF-5) scores and PLNES were evaluated after 6 months and 12 months of treatment. Sexual Encounter Profile (SEP-Question 2 and SEP-Question 3) were evaluated after 12 months of treatment. Ninety-one of the 100 randomized patients completed the study. We found that the 5 mg tadalafil once a day (OaD) combined with VED can help improve IIEF-5 scores in nsRP patients after both 6 months and 12 months. VED alone or combined with tadalafil OaD can help patients maintain PLNES. VED combined with tadalafil OaD can improve the rate of successful penetration (SEP-Question 2) after 12 months. There were no significant differences in the return to target EF after 12 months among the groups. No significant correlation was noted between the variables and return to target EF (IIEF ≥ 17), and between the variables and effective shortening of the patient's penis (shortening ≥ 1 cm) after 12 months of intervention.
海绵体神经损伤是勃起功能障碍(ED)的一个重要原因。尽管保护神经技术已广泛应用于保留神经的根治性前列腺切除术(nsRP)中,但手术后 ED 的发生率仍然很高。我们的研究目的是评估 nsRP 后计划使用磷酸二酯酶 5 抑制剂(PDE5i)、真空勃起装置(VED)治疗和联合治疗后的勃起功能(EF)和非勃起状态下的阴茎长度(PLNES)。100 例局限性前列腺癌且 EF 正常的患者被随机分为计划 PDE5i 组、VED 治疗组、联合治疗组和无任何干预的对照组。在治疗 6 个月和 12 个月后评估国际勃起功能指数-5(IIEF-5)评分和 PELNS,在治疗 12 个月后评估性遭遇概况(SEP-Question 2 和 SEP-Question 3)。100 例随机患者中有 91 例完成了研究。我们发现,5 毫克他达拉非每日一次(OaD)联合 VED 可以帮助 nsRP 患者在治疗 6 个月和 12 个月后提高 IIEF-5 评分。VED 单独或与他达拉非 OaD 联合使用可以帮助患者维持 PELNS。VED 联合他达拉非 OaD 可以提高 12 个月后的成功插入率(SEP-Question 2)。治疗 12 个月后,各组的目标 EF 恢复率没有差异。12 个月的干预后,变量与目标 EF(IIEF≥17)的恢复以及变量与患者阴茎有效缩短(缩短≥1cm)之间没有显著相关性。