Fauss Gizelle N K, Strain Misty M, Huang Yung-Jen, Reynolds Joshua A, Davis Jacob A, Henwood Melissa K, West Christopher R, Grau James W
Department of Psychological and Brain Sciences, Texas A&M University, College Station, TX, United States.
Department of Cellular and Integrative Physiology, University of Texas Health Science San Antonio, San Antonio, TX, United States.
Front Syst Neurosci. 2021 Dec 15;15:733056. doi: 10.3389/fnsys.2021.733056. eCollection 2021.
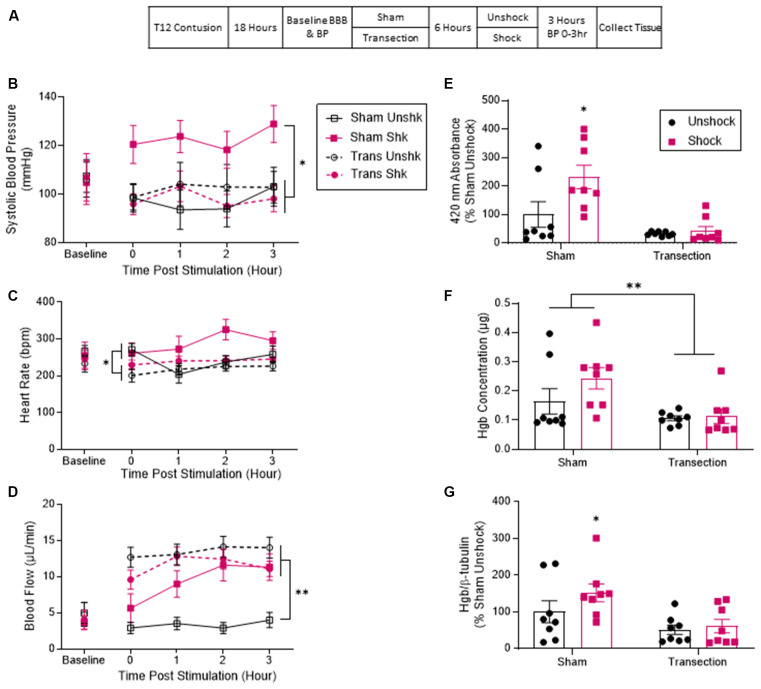
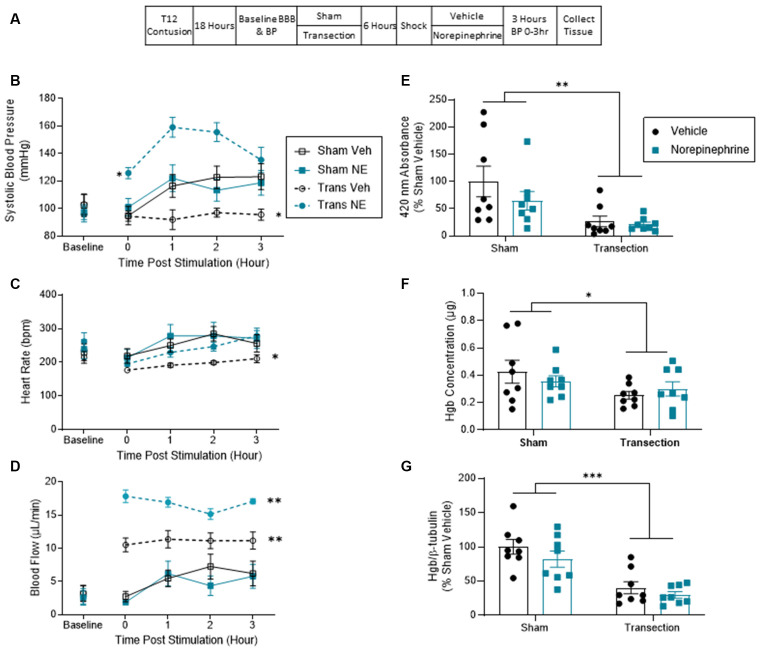
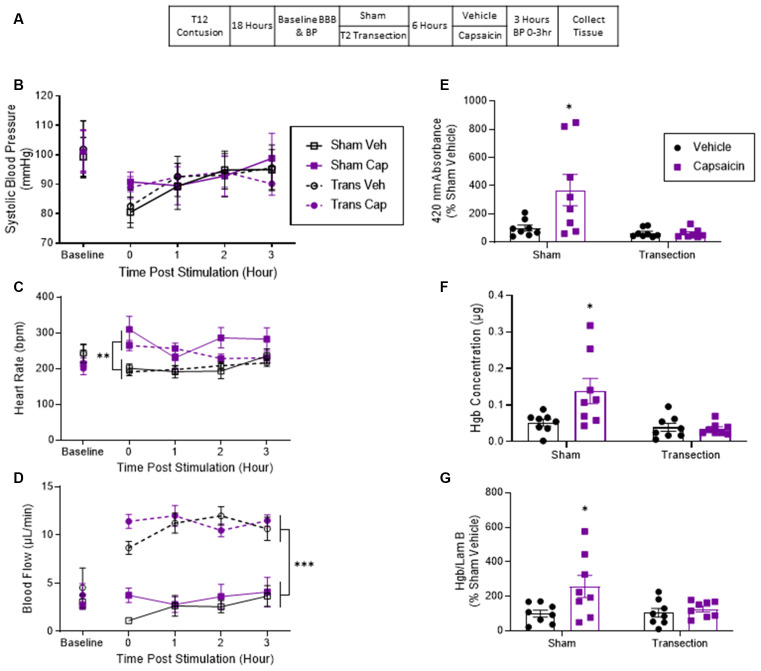
Pain (nociceptive) input soon after spinal cord injury (SCI) expands the area of tissue loss (secondary injury) and impairs long-term recovery. Evidence suggests that nociceptive stimulation has this effect because it promotes acute hemorrhage. Disrupting communication with the brain blocks this effect. The current study examined whether rostral systems exacerbate tissue loss because pain input drives an increase in systolic blood pressure (BP) and flow that fuels blood infiltration. Rats received a moderate contusion injury to the lower thoracic (T12) spinal cord. Communication with rostral processes was disrupted by cutting the spinal cord 18 h later at T2. Noxious electrical stimulation (shock) applied to the tail (Experiment 1), or application of the irritant capsaicin to one hind paw (Experiment 2), increased hemorrhage at the site of injury. Shock, but not capsaicin, increased systolic BP and tail blood flow in sham-operated rats. Cutting communication with the brain blocked the shock-induced increase in systolic BP and tail blood flow. Experiment 3 examined the effect of artificially driving a rise in BP with norepinephrine (NE) in animals that received shock. Spinal transection attenuated hemorrhage in vehicle-treated rats. Treatment with NE drove a robust increase in BP and tail blood flow but did not increase the extent of hemorrhage. The results suggest pain input after SCI can engage rostral processes that fuel hemorrhage and drive sustained cardiovascular output. An increase in BP was not, however, necessary or sufficient to drive hemorrhage, implicating other brain-dependent processes.
脊髓损伤(SCI)后不久的疼痛(伤害性)输入会扩大组织损失(继发性损伤)的范围,并损害长期恢复。有证据表明,伤害性刺激具有这种作用是因为它会促进急性出血。中断与大脑的通讯可阻止这种作用。当前的研究调查了延髓系统是否会加剧组织损失,因为疼痛输入会导致收缩压(BP)升高和血流量增加,从而加剧血液浸润。给大鼠的下胸段(T12)脊髓造成中度挫伤。18小时后在T2处切断脊髓,从而中断与延髓的通讯。对尾巴施加有害电刺激(电击)(实验1),或在后爪之一上涂抹刺激性辣椒素(实验2),会增加损伤部位的出血。在假手术大鼠中,电击而非辣椒素会增加收缩压和尾巴血流量。切断与大脑的通讯可阻止电击引起的收缩压和尾巴血流量增加。实验3研究了在接受电击的动物中用去甲肾上腺素(NE)人为地使血压升高的影响。脊髓横断可减轻接受赋形剂治疗的大鼠的出血。用NE治疗可使血压和尾巴血流量大幅增加,但不会增加出血程度。结果表明,SCI后的疼痛输入可激活延髓过程,从而加剧出血并驱动持续的心血管输出。然而,血压升高并非驱动出血的必要或充分条件,这意味着存在其他依赖大脑的过程。