Xiang Yan-Jun, Wang Kang, Zheng Yi-Tao, Yu Hong-Ming, Cheng Yu-Qiang, Wang Wei-Jun, Shan Yun-Feng, Cheng Shu-Qun
Department of Hepatobiliary Surgery, The First Affiliated Hospital, Wenzhou Medical University, Wenzhou, China.
Department of Hepatic Surgery VI, Eastern Hepatobiliary Surgery Hospital, Second Military Medical University, Shanghai, China.
Front Oncol. 2021 Dec 16;11:726569. doi: 10.3389/fonc.2021.726569. eCollection 2021.
Microvascular invasion (MVI) is a significant risk factor affecting survival outcomes of patients after R0 liver resection (LR) for hepatocellular carcinoma (HCC). However, whether the existing staging systems of hepatocellular carcinoma can distinguish the prognosis of patients with MVI and the prognostic value of MVI in different subtypes of hepatocellular carcinoma remains to be clarified.
A dual-center retrospective data set of 1,198 HCC patients who underwent R0 LR was included in the study between 2014 and 2016. Baseline characteristics and staging information were collected. Homogeneity and modified Akaike information criterion (AICc) were compared between each system. And the prognostic significance of MVI for overall survival (OS) was studied in each subgroup.
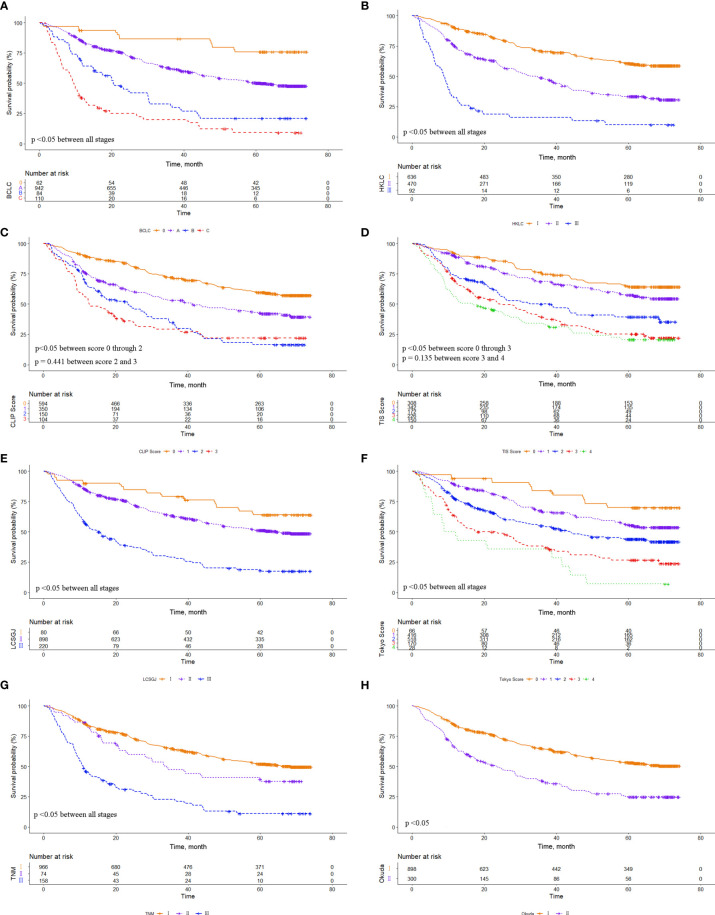
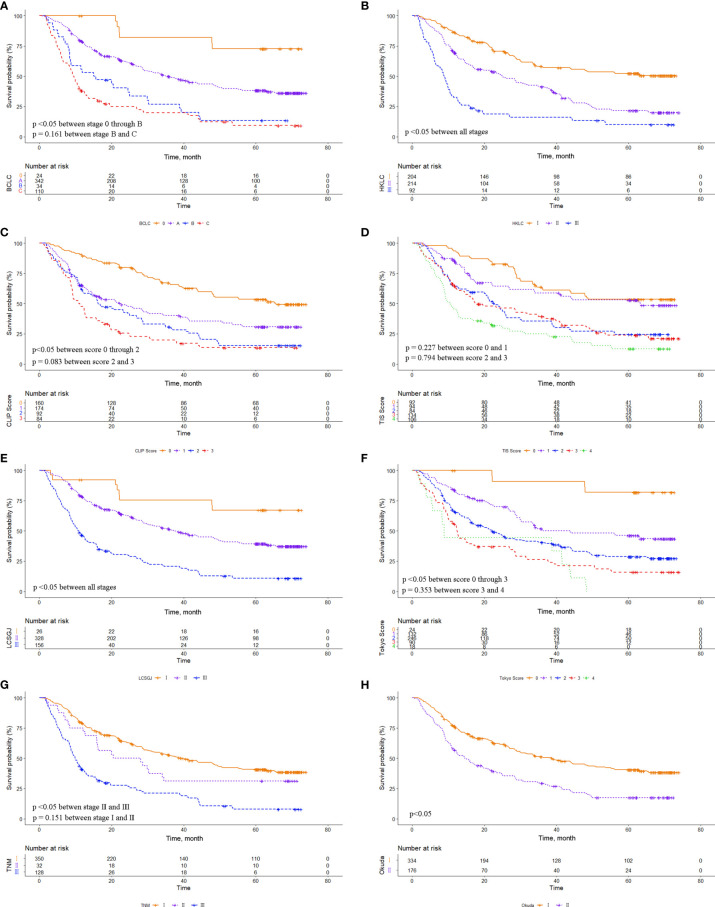
In the entire cohort, there were no significant survival differences between Cancer of the Liver Italian Program (CLIP) score 2 and 3 (p = 0.441), and between Taipei Integrated Scoring System (TIS) score 3 and 4 (p = 0.135). In the MVI cohort, there were no significant survival differences between Barcelona Clinic Liver Cancer stages B and C (p=0.161), CLIP scores 2 and 3 (p = 0.083), TIS scores 0 and 1 (p = 0.227), TIS scores 2 and 3 (p =0.794), Tokyo scores 3 and 4 (p=0.353), and American Joint Committee on Cancer Tumor-Node-Metastasis 7 stage I and II (p=0.151). Among the eight commonly used HCC staging systems, the Hong Kong Liver Cancer (HKLC) staging system showed the highest homogeneity and the lowest AICc value in both the entire cohort and MVI cohort. In each subgroup of the staging systems, MVI generally exhibited poor survival outcomes.
The HKLC staging system was the most accurate model for discriminating the prognosis of MVI patients, among the eight staging systems. Meanwhile, our findings suggest that MVI may be needed to be incorporated into the current HCC staging systems as one of the grading criteria.
微血管侵犯(MVI)是影响肝细胞癌(HCC)患者行R0肝切除(LR)后生存结局的重要危险因素。然而,现有的肝细胞癌分期系统能否区分MVI患者的预后以及MVI在不同亚型肝细胞癌中的预后价值仍有待阐明。
纳入2014年至2016年间1198例行R0 LR的HCC患者的双中心回顾性数据集。收集基线特征和分期信息。比较各系统之间的同质性和修正赤池信息准则(AICc)。并在每个亚组中研究MVI对总生存期(OS)的预后意义。
在整个队列中,意大利肝癌项目(CLIP)评分2和3之间(p = 0.441)以及台北综合评分系统(TIS)评分3和4之间(p = 0.135)无显著生存差异。在MVI队列中,巴塞罗那临床肝癌分期B和C之间(p = 0.161)、CLIP评分2和3之间(p = 0.083)、TIS评分0和1之间(p = 0.227)、TIS评分2和3之间(p = 0.794)、东京评分3和4之间(p = 0.353)以及美国癌症联合委员会肿瘤-淋巴结-转移7期I和II之间(p = 0.151)无显著生存差异。在八个常用的HCC分期系统中,香港肝癌(HKLC)分期系统在整个队列和MVI队列中均显示出最高的同质性和最低的AICc值。在分期系统的每个亚组中,MVI通常表现出生存结局较差。
在八个分期系统中,HKLC分期系统是区分MVI患者预后的最准确模型。同时,我们的研究结果表明,可能需要将MVI纳入当前的HCC分期系统作为分级标准之一。