Webster Jonathan A, Luznik Leo, Gojo Ivana
Hematologic Malignancies and Bone Marrow Transplantation Program, Department of Oncology, Johns Hopkins University School of Medicine, Baltimore, MD, United States.
Front Oncol. 2021 Dec 16;11:812207. doi: 10.3389/fonc.2021.812207. eCollection 2021.
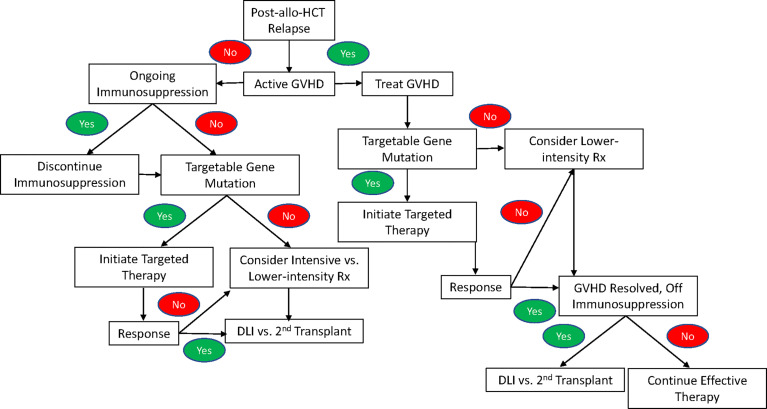
With advances in allogeneic hematopoietic stem cell transplant (allo-HCT), disease relapse has replaced transplant-related mortality as the primary cause of treatment failure for patients with acute myeloid leukemia (AML). The efficacy of allo-HCT in AML is a consequence of a graft-versus-leukemia (GVL) effect that is mediated by T lymphocytes, and unique mechanisms of immune evasion underlying post-allo-HCT AML relapses have recently been characterized. Relapsed AML following allo-HCT presents a particularly vexing clinical challenge because transplant-related toxicities, such as graft-versus-host (GVHD) and infections, increase the risk of treatment-related morbidity and mortality. In general, the prognosis of relapsed AML following allo-HCT is poor with most patients failing to achieve a subsequent remission and 2-year survival consistently <15%. The two factors that have been found to predict a better prognosis are a longer duration of post-transplant remission prior to relapse and a lower disease burden at the time of relapse. When considered in combination with a patient's age; co-morbidities; and performance status, these factors can help to inform the appropriate therapy for the treatment of post-transplant relapse. This review discusses the options for the treatment of post-transplant AML relapse with a focus on the options to achieve a subsequent remission and consolidation with cellular immunotherapy, such as a second transplant or donor lymphocyte infusion (DLI). While intensive reinduction therapy and less intensive approaches with hypomethylating agents have long represented the two primary options for the initial treatment of post-transplant relapse, molecularly targeted therapies and immunotherapy are emerging as potential alternative options to achieve remission. Herein, we highlight response and survival outcomes achieved specifically in the post-transplant setting using each of these approaches and discuss how some therapies may overcome the immunologic mechanisms that have been implicated in post-transplant relapse. As long-term survival in post-transplant relapse necessarily involves consolidation with cellular immunotherapy, we present data on the efficacy and toxicity of both DLI and second allo-HCT including when such therapies are integrated with reinduction. Finally, we provide our general approach to the treatment of post-transplant relapse, integrating both novel therapies and our improved understanding of the mechanisms underlying post-transplant relapse.
随着异基因造血干细胞移植(allo-HCT)技术的进步,疾病复发已取代移植相关死亡率,成为急性髓系白血病(AML)患者治疗失败的主要原因。allo-HCT治疗AML的疗效源于T淋巴细胞介导的移植物抗白血病(GVL)效应,并且最近已经明确了allo-HCT后AML复发所潜在的独特免疫逃逸机制。allo-HCT后复发的AML带来了特别棘手的临床挑战,因为移植相关毒性,如移植物抗宿主病(GVHD)和感染,增加了治疗相关的发病率和死亡率。一般来说,allo-HCT后复发的AML预后较差,大多数患者无法获得后续缓解,2年生存率始终低于15%。已发现的两个预后较好的预测因素是复发前移植后缓解持续时间较长以及复发时疾病负担较低。结合患者的年龄、合并症和体能状态考虑,这些因素有助于为移植后复发的治疗选择合适的疗法。本综述讨论了移植后AML复发的治疗选择,重点是通过细胞免疫疗法实现后续缓解和巩固的选择,如第二次移植或供体淋巴细胞输注(DLI)。虽然强化再诱导治疗和使用低甲基化药物的强度较低的方法长期以来一直是移植后复发初始治疗的两种主要选择,但分子靶向治疗和免疫治疗正作为实现缓解的潜在替代选择出现。在此,我们重点介绍使用每种方法在移植后环境中具体实现的缓解和生存结果,并讨论一些疗法如何克服与移植后复发相关的免疫机制。由于移植后复发的长期生存必然涉及细胞免疫疗法的巩固,我们展示了DLI和第二次allo-HCT的疗效和毒性数据,包括这些疗法与再诱导联合使用时的情况。最后,我们提供了我们治疗移植后复发的一般方法,整合了新疗法以及我们对移植后复发潜在机制的深入理解。