Department of Rheumatology, Leiden University Medical Centre, Leiden, the Netherlands.
Department of Rheumatology, Erasmus Medical Centre, Rotterdam, the Netherlands.
Arthritis Res Ther. 2022 Jan 3;24(1):4. doi: 10.1186/s13075-021-02671-z.
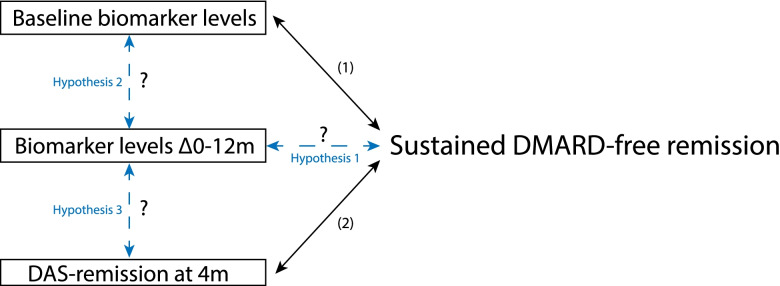
Rheumatoid arthritis (RA) is a heterogeneous disease, as evidenced by the differences in long-term outcomes. This applies especially to anti-citrullinated protein antibodies (ACPA)-negative RA, where a proportion achieves sustained DMARD-free remission (SDFR; sustained absence of synovitis after DMARD cessation). Differentiation of RA patients who will achieve SDFR can guide personalized treatment/tapering strategies. Although this subgroup remains scarcely discerned, previous research demonstrated that these RA patients are characterized by an early clinical response (DAS remission after 4 months) after DMARD start. We studied whether, in addition to this clinical response, a specific biomarker response can further distinguish the subgroup of RA patients most likely to achieve SDFR.
In 266 RA patients, levels of 12 biomarkers (SAA/CRP/MMP-1/MMP-3/resistin/leptin/IL-6/TNF-R1/YKL-40/EGF/VEGF/VCAM-1), in the first 2 years after diagnosis, were studied in relation to SDFR, stratified for ACPA status. Subsequently, biomarkers associated with SDFR development were combined with early DAS remission to study its additional value in defining subgroups. Since most biomarker levels are not routinely measured in clinical practice, we explored how this subgroup can be clinically recognized.
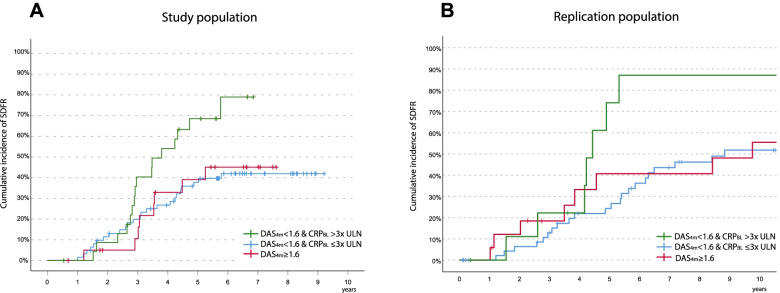
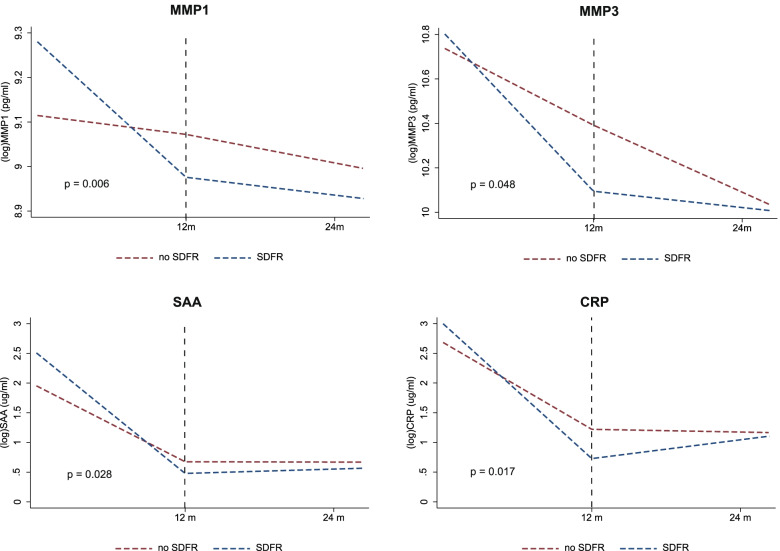
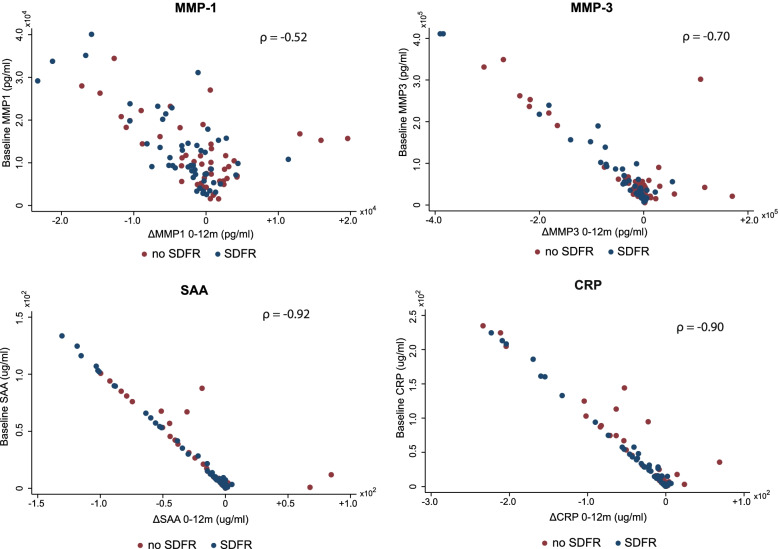
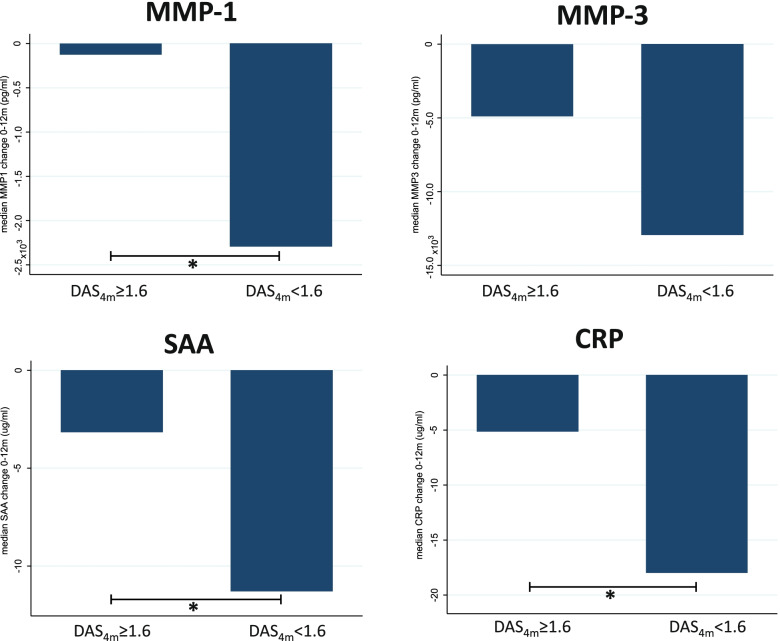
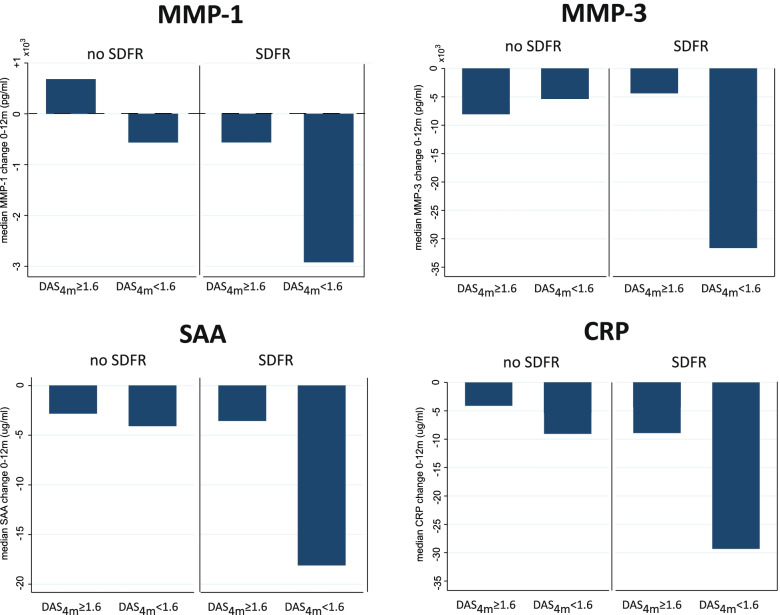
ACPA-negative RA patients achieving SDFR were characterized by high baseline levels and stronger decline in MMP-1/MMP-3/SAA/CRP after DMARD-start, respectively 1.30×/1.44×/2.12×/2.24× stronger. This effect was absent in ACPA-positive RA. In ACPA-negative RA, a strong biomarker decline is associated with early DAS remission. The combination of both declines (clinical, biomarker) was present in a subgroup of ACPA-negative RA patients achieving SDFR. This subgroup can be clinically recognized by the combination of high baseline CRP levels (≥ 3 times ULN), and early DAS remission (DAS < 1.6). This latter was replicated in independent ACPA-negative RA patients.
ACPA-negative RA patients with early DAS remission and a strong biomarker response (or baseline CRP levels ≥ 3× ULN) are most likely to achieve SDFR later on. This could guide personalized decisions on DMARD tapering/cessation in ACPA-negative RA.
类风湿关节炎(RA)是一种异质性疾病,这表现在长期预后的差异上。这尤其适用于抗瓜氨酸化蛋白抗体(ACPA)阴性 RA,其中一部分患者可达到持续的 DMARD 无缓解(DMARD 停药后持续无滑膜炎)。区分可能达到持续无缓解的 RA 患者可以指导个体化治疗/逐渐减少策略。尽管这一亚组仍难以识别,但先前的研究表明,这些 RA 患者的特征是在 DMARD 开始后 4 个月达到 DAS 缓解。我们研究了除了这种临床反应外,特定的生物标志物反应是否可以进一步区分最有可能达到持续无缓解的 RA 患者亚组。
在 266 例 RA 患者中,研究了在诊断后的前 2 年内,12 种生物标志物(SAA/CRP/MMP-1/MMP-3/抵抗素/瘦素/IL-6/TNF-R1/YKL-40/EGF/VEGF/VCAM-1)的水平与 SDFR 的关系,按 ACPA 状态分层。随后,将与 SDFR 发展相关的生物标志物与早期 DAS 缓解相结合,以研究其在定义亚组方面的额外价值。由于大多数生物标志物水平在临床实践中并未常规测量,我们探讨了如何通过临床识别该亚组。
达到持续无缓解的 ACPA 阴性 RA 患者的基线水平较高,且在 DMARD 开始后 MMP-1/MMP-3/SAA/CRP 的下降幅度更大,分别为 1.30×/1.44×/2.12×/2.24×。在 ACPA 阳性 RA 中则不存在这种现象。在 ACPA 阴性 RA 中,生物标志物的强烈下降与早期 DAS 缓解相关。在达到持续无缓解的 ACPA 阴性 RA 患者亚组中存在两者下降(临床和生物标志物)的结合。该亚组可通过高基线 CRP 水平(≥ 3 倍 ULN)和早期 DAS 缓解(DAS<1.6)相结合来识别。在独立的 ACPA 阴性 RA 患者中也得到了验证。
具有早期 DAS 缓解和强烈生物标志物反应(或基线 CRP 水平≥3×ULN)的 ACPA 阴性 RA 患者最有可能在以后达到持续无缓解。这可以指导 ACPA 阴性 RA 患者 DMARD 逐渐减少/停药的个体化决策。