McCarthy Caroline, Clyne Barbara, Smith Susan M, Boland Fiona, Wallace Emma, Flood Michelle, Moriarty Frank
Department of General Practice, RCSI University of Medicine and Health Sciences, 123 St Stephen's Green, Dublin D02 YN77, Ireland.
Department of Public Health & Epidemiology, School of Population Health, RCSI University of Medicine and Health Sciences, 123 St Stephen's Green, Dublin D02 YN77, Ireland.
Fam Pract. 2025 Jun 4;42(4). doi: 10.1093/fampra/cmaf056.
Multimorbidity guidelines recommend tailoring care to patients' priorities. The Supporting Prescribing in Multimorbidity in Primary Care (SPPiRE) trial focused on optimizing medicines use in older adults with significant polypharmacy and tailoring prescribing and deprescribing to individual priorities. This study aimed to compare self-reported and general practitioner (GP)-recorded patient priorities and examine the impact of prioritizing pain on analgesic prescribing.
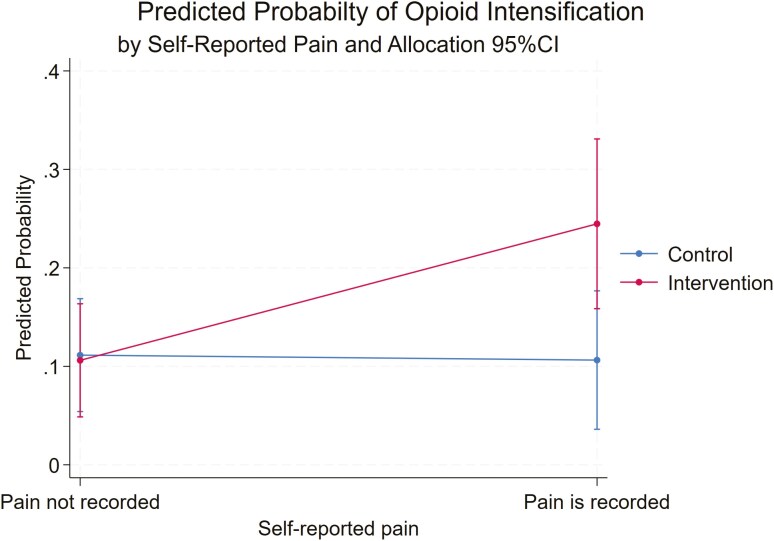
This secondary cohort analysis of the SPPIRE trial and process evaluation assessed baseline participant-identified priorities and intervention group GP-recorded priorities during medication reviews with agreement assessed using Cohen's kappa. Analgesic prescribing patterns and daily morphine milligram equivalents changes during the study period were summarized. The impact of pain (self-reported, GP-recorded, and severe or extreme pain on the baseline EQ5D) on opioid intensification was analysed using multi-level models accounting for GP practice clustering and intervention effects.
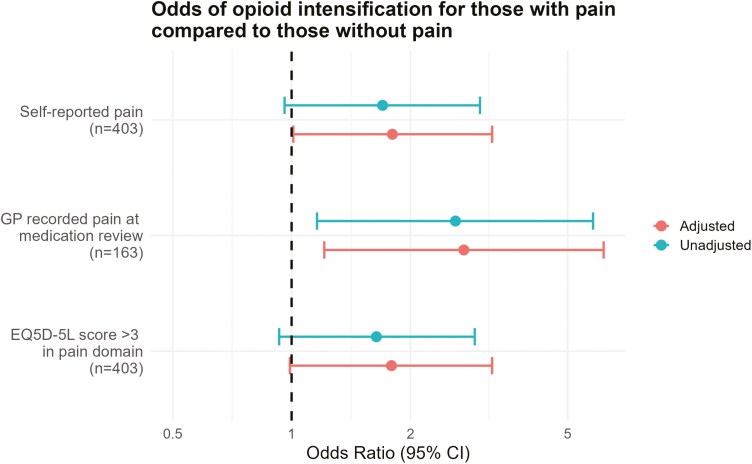
A total of 403 patients (mean age 76.5 years) were included; 178 (44.2%) reported pain as a priority at baseline. Agreement between self-reported and GP-recorded pain was poor (kappa 0.118, P = 0.05). Most analgesic prescriptions decreased during the study, except for potent opioids, which increased in both trial arms. All three pain variables were associated with increased odds of opioid intensification at follow-up.
In this older population of patients with significant polypharmacy, identifying pain as a priority was associated with an increased likelihood of opioid intensification, despite guidelines advising against their use for chronic pain. This study highlights the challenges faced by GPs treating pain in older adults with multimorbidity.
多重疾病指南建议根据患者的优先事项提供个性化护理。初级保健中多重疾病支持处方(SPPiRE)试验的重点是优化患有严重多重用药的老年人的药物使用,并根据个人优先事项调整处方和减药。本研究旨在比较患者自我报告的和全科医生(GP)记录的优先事项,并研究将疼痛列为优先事项对镇痛药处方的影响。
本对SPPiRE试验的二次队列分析和过程评估在药物审查期间评估了参与者在基线时确定的优先事项以及干预组GP记录的优先事项,并使用Cohen's kappa评估一致性。总结了研究期间镇痛药的处方模式和每日吗啡毫克当量的变化。使用考虑GP诊所聚类和干预效果的多层次模型分析了疼痛(自我报告、GP记录以及基线EQ5D上的严重或极度疼痛)对阿片类药物强化的影响。
共纳入403例患者(平均年龄76.5岁);178例(44.2%)在基线时将疼痛列为优先事项。自我报告的疼痛与GP记录的疼痛之间的一致性较差(kappa为0.118,P = 0.05)。在研究期间,大多数镇痛药处方减少,但强效阿片类药物除外,两个试验组中的强效阿片类药物处方均增加。所有三个疼痛变量均与随访时阿片类药物强化的几率增加相关。
在这个患有严重多重用药的老年患者群体中,将疼痛列为优先事项与阿片类药物强化的可能性增加相关,尽管指南不建议将其用于慢性疼痛。本研究凸显了全科医生在治疗患有多重疾病的老年人疼痛时所面临的挑战。