Tufts Friedman School of Nutrition Science and Policy, Boston, Massachusetts.
Midwest Biomedical Research, Addison, Illinois.
JAMA Netw Open. 2022 Jan 4;5(1):e2141898. doi: 10.1001/jamanetworkopen.2021.41898.
Intense interest exists in novel ω-3 formulations with high bioavailability to reduce blood triglyceride (TG) levels.
To determine the phase 3 efficacy and safety of a naturally derived krill oil with eicosapentaenoic acid and docosahexaenoic acid as both phospholipid esters (PLs) and free fatty acids (FFAs) (ω-3-PL/FFA [CaPre]), measured by fasting TG levels and other lipid parameters in severe hypertriglyceridemia.
DESIGN, SETTING, AND PARTICIPANTS: This study pooled the results of 2 identical randomized, double-blind, placebo-controlled trials. TRILOGY 1 (Study of CaPre in Lowering Very High Triglycerides) enrolled participants at 71 US centers from January 23, 2018, to November 20, 2019; TRILOGY 2 enrolled participants at 93 US, Canadian, and Mexican centers from April 6, 2018, to January 9, 2020. Patients with fasting TG levels from 500 to 1500 mg/dL, with or without stable treatment with statins, fibrates, or other agents to lower cholesterol levels, were eligible to participate.
Randomization (2.5:1.0) to ω-3-PL/FFA, 4 g/d, vs placebo (cornstarch) for 26 weeks.
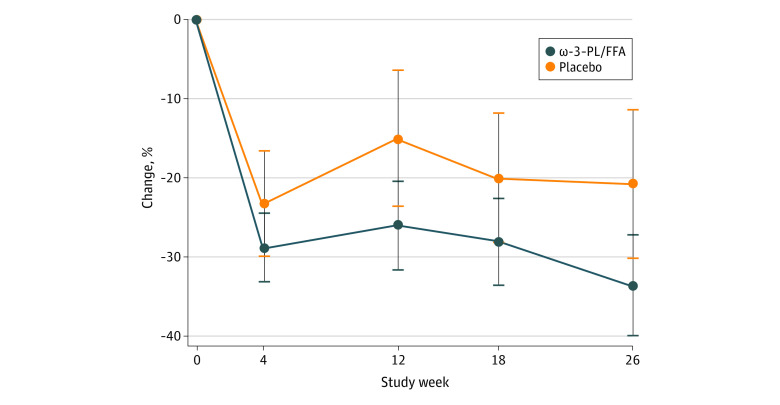
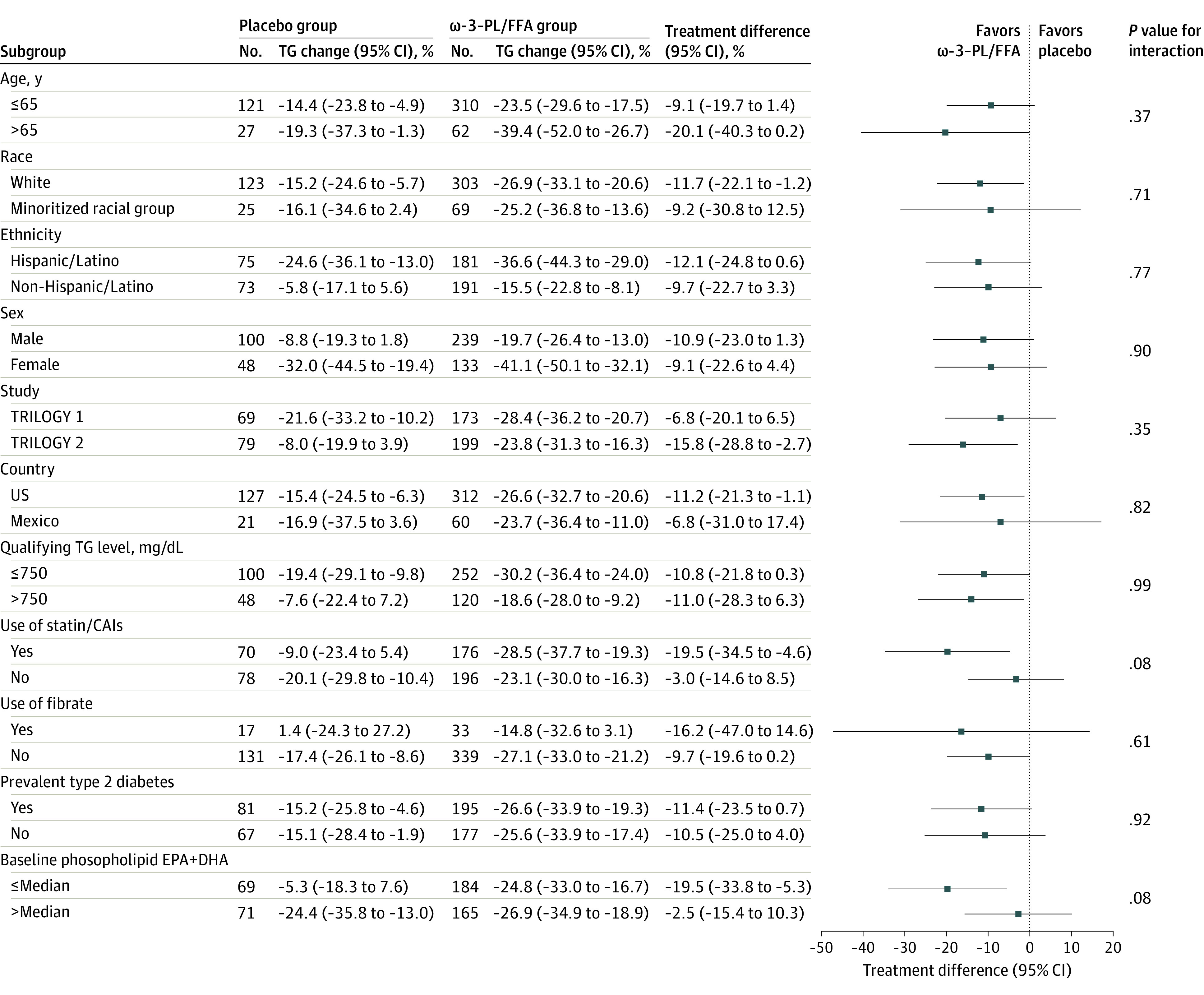
The primary outcome was the mean percentage of change in TG levels at 12 weeks; persistence at 26 weeks was the key secondary outcome. Other prespecified secondary outcomes were effects on levels of non-high-density lipoprotein cholesterol (non-HDL-C), very-low-density lipoprotein cholesterol (VLDL-C), HDL-C, and low-density lipoprotein cholesterol (LDL-C); safety and tolerability; and TG level changes in prespecified subgroups.
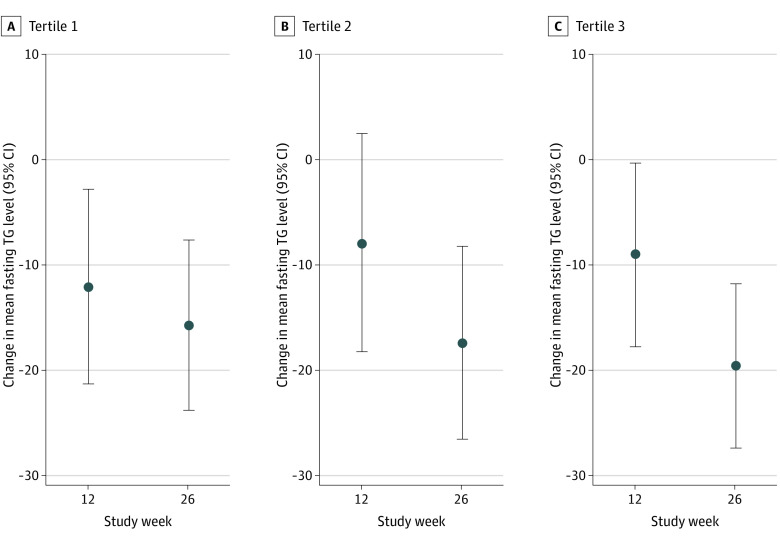
A total of 520 patients were randomized, with a mean (SD) age of 54.9 (11.2) years (339 men [65.2%]), mean (SD) body mass index of 31.5 (5.1), and baseline mean (SD) TG level of 701 (222) mg/dL. Two hundred fifty-six patients (49.2%) were of Hispanic or Latino ethnicity; 275 (52.9%) had diabetes; and 248 (47.7%) were receiving statins. In the intention-to-treat analysis, TG levels were reduced by 26.0% (95% CI, 20.5%-31.5%) in the ω-3-PL/FFA group and 15.1% (95% CI, 6.6%-23.5%) in the placebo group at 12 weeks (mean treatment difference, -10.9% [95% CI, -20.4% to -1.5%]; P = .02), with reductions persisting at 26 weeks (mean treatment difference, -12.7% [95% CI, -23.1% to -2.4%]; P = .02). Compared with placebo, ω-3-PL/FFA had no significant effect at 12 weeks on mean treatment differences for non-HDL-C (-3.2% [95% CI, -8.0% to 1.6%]; P = .18), VLDL-C (-3.8% [95% CI, -12.2% to 4.7%]; P = .38), HDL-C (0.7% [95% CI, -3.7% to 5.1%]; P = .77), or LDL-C (4.5% [95% CI, -5.9% to 14.8%]; P = .40) levels; corresponding differences at 26 weeks were -5.8% (95% CI, -11.3% to -0.3%; P = .04) for non-HDL-C levels, -9.1% (95% CI, -21.5% to 3.2%; P = .15) for VLDL-C levels, 1.9% (95% CI, -4.8% to 8.6%; P = .57) for HDL-C levels, and 6.3% (95% CI, -12.4% to 25.0%; P = .51) for LDL-C levels. Effects on the primary end point did not vary significantly by age, sex, race and ethnicity, country, qualifying TG level, diabetes, or fibrate use but tended to be larger among patients taking statins or cholesterol absorption inhibitors at baseline (mean treatment difference, -19.5% [95% CI, -34.5% to -4.6%]; P = .08 for interaction) and with lower (less than median) baseline blood eicosapentaenoic acid plus docosahexaenoic acid levels (-19.5% [95% CI, -33.8% to -5.3%]; P = .08 for interaction). ω-3-PL/FFA was well tolerated, with a safety profile similar to that of placebo.
This study found that ω-3 -PL/FFA, a novel krill oil-derived ω-3 formulation, reduced TG levels and was safe and well tolerated in patients with severe hypertriglyceridemia.
ClinicalTrials.gov Identifiers: NCT03398005 and NCT03361501.
人们对具有高生物利用度的新型 ω-3 制剂非常感兴趣,以降低血液甘油三酯 (TG) 水平。
评估天然来源的磷虾油中二十碳五烯酸 (EPA) 和二十二碳六烯酸 (DHA) 同时作为磷脂酯 (PL) 和游离脂肪酸 (FFA) (ω-3-PL/FFA [CaPre]) 的降 TG 疗效和安全性,用空腹 TG 水平和其他血脂参数衡量重度高甘油三酯血症患者的疗效。
设计、地点和参与者:本研究汇集了两项完全相同的随机、双盲、安慰剂对照试验的结果。TRILOGY 1(研究 CaPre 降低极高 TG)于 2018 年 1 月 23 日至 2019 年 11 月 20 日在 71 个美国中心招募参与者;TRILOGY 2 于 2018 年 4 月 6 日至 2020 年 1 月 9 日在美国、加拿大和墨西哥的 93 个中心招募参与者。入选标准为空腹 TG 水平为 500-1500mg/dL,且正在稳定接受他汀类药物、贝特类药物或其他降胆固醇药物治疗。
随机分配(2.5:1.0)至 ω-3-PL/FFA,4g/d,或安慰剂(玉米淀粉),疗程 26 周。
主要结局为 12 周时 TG 水平的平均百分比变化;26 周时的持续缓解是关键次要结局。其他预定的次要结局为非高密度脂蛋白胆固醇 (non-HDL-C)、极低密度脂蛋白胆固醇 (VLDL-C)、高密度脂蛋白胆固醇 (HDL-C)和低密度脂蛋白胆固醇 (LDL-C)水平的影响;安全性和耐受性;以及特定亚组中 TG 水平的变化。
共纳入 520 名患者,平均(SD)年龄为 54.9(11.2)岁(339 名男性[65.2%]),平均(SD)体重指数为 31.5(5.1),基线平均(SD)TG 水平为 701(222)mg/dL。256 名患者(49.2%)为西班牙裔或拉丁裔;275 名(52.9%)患有糖尿病;248 名(47.7%)正在服用他汀类药物。在意向治疗分析中,ω-3-PL/FFA 组 TG 水平降低 26.0%(95%CI,20.5%-31.5%),安慰剂组降低 15.1%(95%CI,6.6%-23.5%),12 周时平均治疗差异为-10.9%(95%CI,-20.4%至-1.5%);P=0.02),26 周时仍有降低(平均治疗差异,-12.7% [95% CI,-23.1% 至 -2.4%];P=0.02)。与安慰剂相比,ω-3-PL/FFA 对 12 周时非高密度脂蛋白胆固醇(-3.2% [95% CI,-8.0% 至 1.6%];P=0.18)、VLDL-C(-3.8% [95% CI,-12.2% 至 4.7%];P=0.38)、HDL-C(0.7% [95% CI,-3.7% 至 5.1%];P=0.77)或 LDL-C(4.5% [95% CI,-5.9% 至 14.8%])水平的平均治疗差异无显著影响;26 周时的差异分别为-5.8%(95% CI,-11.3% 至 -0.3%)、-9.1%(95% CI,-21.5% 至 3.2%)、1.9%(95% CI,-4.8% 至 8.6%)和 6.3%(95% CI,-12.4% 至 25.0%);这些差异与年龄、性别、种族和民族、国家、TG 水平、糖尿病或是否使用贝特类药物无关,但在基线时使用他汀类药物或胆固醇吸收抑制剂的患者中(平均治疗差异,-19.5% [95% CI,-34.5% 至 -4.6%];P=0.08 用于交互作用)和基线时血液中二十碳五烯酸加二十二碳六烯酸水平较低(低于中位数)的患者中(-19.5% [95% CI,-33.8% 至 -5.3%];P=0.08 用于交互作用)较大。ω-3-PL/FFA 耐受性良好,安全性与安慰剂相似。
本研究发现,新型磷虾油衍生的 ω-3 制剂 ω-3-PL/FFA 可降低 TG 水平,在重度高甘油三酯血症患者中安全且耐受性良好。
ClinicalTrials.gov 标识符:NCT03398005 和 NCT03361501。