CDC Foundation, Atlanta, USA.
Harvard Medical School, Boston, USA.
Hum Resour Health. 2022 Jan 6;20(1):1. doi: 10.1186/s12960-021-00683-z.
Although supervision is a ubiquitous approach to support health programs and improve health care provider (HCP) performance in low- and middle-income countries (LMICs), quantitative evidence of its effects is unclear. The objectives of this study are to describe the effect of supervision strategies on HCP practices in LMICs and to identify attributes associated with greater effectiveness of routine supervision.
We performed a secondary analysis of data on HCP practice outcomes (e.g., percentage of patients correctly treated) from a systematic review on improving HCP performance. The review included controlled trials and interrupted time series studies. We described distributions of effect sizes (defined as percentage-point [%-point] changes) for each supervision strategy. To identify attributes associated with supervision effectiveness, we performed random-effects linear regression modeling and examined studies that directly compared different approaches of routine supervision.
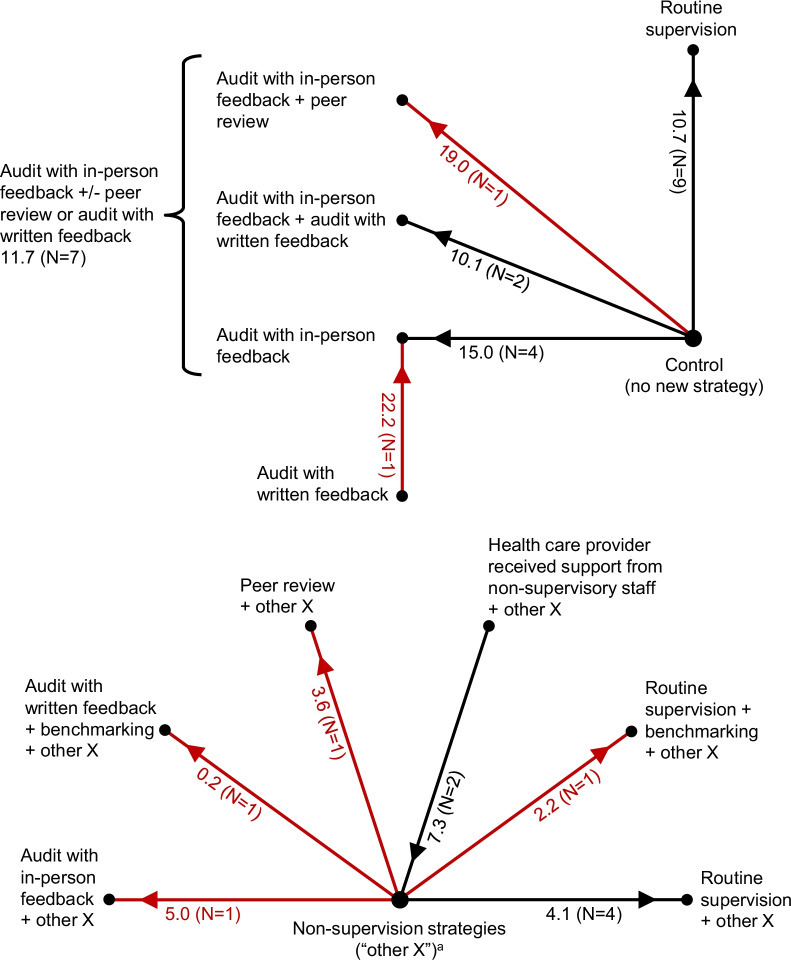
We analyzed data from 81 studies from 36 countries. For professional HCPs, such as nurses and physicians, primarily working at health facilities, routine supervision (median improvement when compared to controls: 10.7%-points; IQR: 9.9, 27.9) had similar effects on HCP practices as audit with feedback (median improvement: 10.1%-points; IQR: 6.2, 23.7). Two attributes were associated with greater mean effectiveness of routine supervision (p < 0.10): supervisors received supervision (by 8.8-11.5%-points), and supervisors participated in problem-solving with HCPs (by 14.2-20.8%-points). Training for supervisors and use of a checklist during supervision visits were not associated with effectiveness. The effects of supervision frequency (i.e., number of visits per year) and dose (i.e., the number of supervision visits during a study) were unclear. For lay HCPs, the effect of routine supervision was difficult to characterize because few studies existed, and effectiveness in those studies varied considerably. Evidence quality for all findings was low primarily because many studies had a high risk of bias.
Although evidence is limited, to promote more effective supervision, our study supports supervising supervisors and having supervisors engage in problem-solving with HCPs. Supervision's integral role in health systems in LMICs justifies a more deliberate research agenda to identify how to deliver supervision to optimize its effect on HCP practices.
尽管监督是一种普遍的方法,可以支持卫生计划并提高中低收入国家(LMIC)卫生保健提供者(HCP)的绩效,但监督效果的定量证据尚不清楚。本研究的目的是描述监督策略对 LMIC 中 HCP 实践的影响,并确定与常规监督更有效相关的属性。
我们对系统评价中关于提高 HCP 绩效的研究中 HCP 实践结果(例如,正确治疗的患者比例)的数据进行了二次分析。该综述包括对照试验和间断时间序列研究。我们描述了每种监督策略的效果大小(定义为百分点[%-point]变化)的分布。为了确定与监督效果相关的属性,我们进行了随机效应线性回归建模,并检查了直接比较常规监督不同方法的研究。
我们分析了来自 36 个国家的 81 项研究的数据。对于主要在卫生设施工作的专业卫生保健人员,如护士和医生,常规监督(与对照组相比的中位数改善:10.7%-points;IQR:9.9,27.9)对 HCP 实践的影响与审核与反馈(中位数改善:10.1%-points;IQR:6.2,23.7)相似。有两个属性与常规监督的平均效果更大相关(p<0.10):监督者接受监督(增加 8.8-11.5%-points),以及监督者与 HCP 一起解决问题(增加 14.2-20.8%-points)。培训监督者和在监督访问期间使用检查表与效果无关。监督频率(即每年的访问次数)和剂量(即研究期间的监督访问次数)的效果尚不清楚。对于非专业卫生保健人员,由于研究较少,常规监督的效果难以描述,而且这些研究中的效果差异很大。所有发现的证据质量都较低,主要是因为许多研究存在较高的偏倚风险。
尽管证据有限,但为了促进更有效的监督,我们的研究支持监督监督者并让监督者与 HCP 一起解决问题。监督在 LMIC 卫生系统中的重要作用证明需要制定更明确的研究议程,以确定如何提供监督以优化其对 HCP 实践的影响。