The Children's Hospital, Faculty of Medicine, Geneva University Hospitals, Geneva, Switzerland.
Pediatric Hematology/Oncology Unit, Faculty of Medicine, Geneva University Hospitals, Geneva, Switzerland.
Front Immunol. 2021 Dec 22;12:773853. doi: 10.3389/fimmu.2021.773853. eCollection 2021.
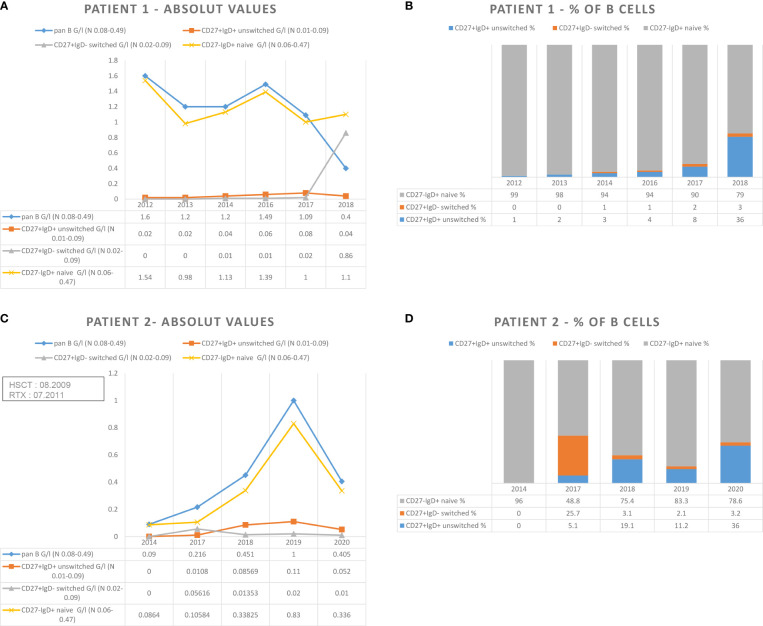
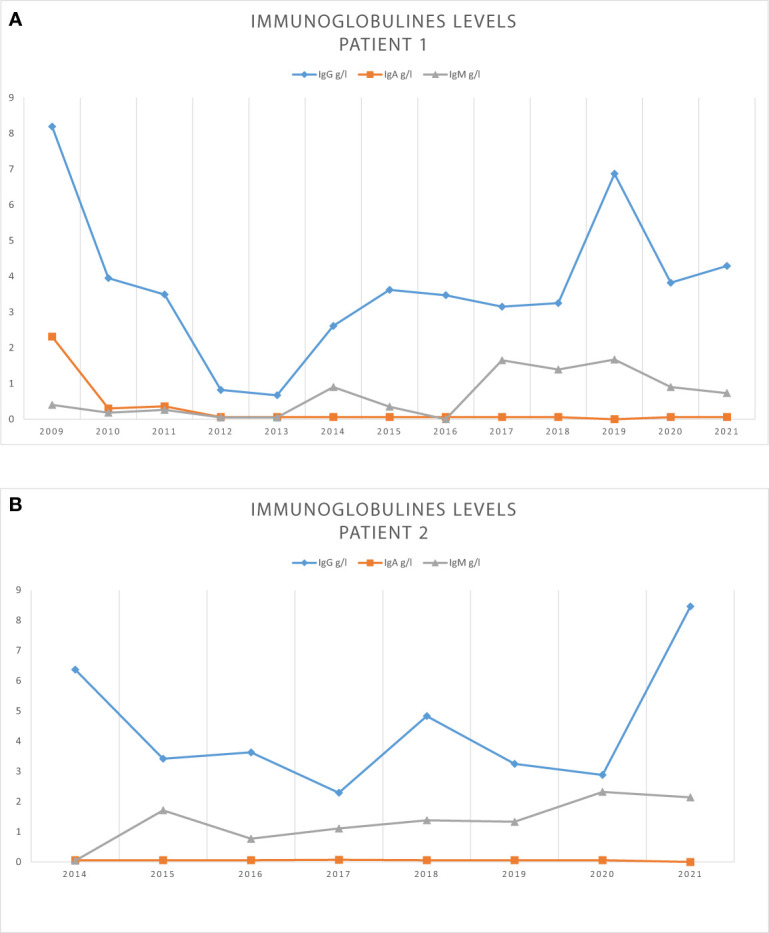
Rituximab (RTX) is an anti-CD20 monoclonal antibody that targets B cells-from the immature pre-B-cell stage in the bone marrow to mature circulating B cells-while preserving stem cells and plasma cells. It is used to treat autoimmune diseases, hematological malignancies, or complications after hematopoietic stem cell transplantation (HSCT). Its safety profile is acceptable; however, a subset of patients can develop persistent hypogammaglobulinemia and associated severe complications, especially in pediatric populations. We report the unrelated cases of two young men aged 17 and 22, presenting with persistent hypogammaglobulinemia more than 7 and 10 years after treatment with RTX, respectively, and administered after HSCT for hemolytic anemia and Epstein-Barr virus reactivation, respectively. Both patients' immunological workups showed low levels of total immunoglobulin, vaccine antibodies, and class switched-memory B cells but an increase in naive B cells, which can also be observed in primary immunodeficiencies such as those making up common variable immunodeficiency. Whole exome sequencing for one of the patients failed to detect a pathogenic variant causing a Mendelian immunological disorder. Annual assessments involving interruption of immunoglobulin replacement therapy each summer failed to demonstrate the recovery of endogenous immunoglobulin production or normal numbers of class switched-memory B cells 7 and 10 years after the patients' respective treatments with RTX. Although the factors that may lead to prolonged hypogammaglobulinemia after rituximab treatment (if necessary) remain unclear, a comprehensive immunological workup before treatment and long-term follow-up are mandatory to assess long-term complications, especially in children.
利妥昔单抗(RTX)是一种抗 CD20 单克隆抗体,可靶向 B 细胞-从骨髓中的未成熟前 B 细胞阶段到成熟循环 B 细胞-同时保留干细胞和浆细胞。它用于治疗自身免疫性疾病、血液系统恶性肿瘤或造血干细胞移植(HSCT)后的并发症。其安全性特征是可以接受的;然而,一部分患者会出现持续性低丙种球蛋白血症和相关严重并发症,尤其是儿科人群。我们报告了两例年轻男性的非相关病例,他们分别在接受 RTX 治疗后 7 年和 10 年以上出现持续性低丙种球蛋白血症,并分别在 HSCT 后因溶血性贫血和 EBV 再激活而接受治疗。两名患者的免疫学检查均显示总免疫球蛋白、疫苗抗体和类别转换记忆 B 细胞水平较低,但幼稚 B 细胞增加,这种情况也可见于原发性免疫缺陷病,如常见可变免疫缺陷病。对其中一名患者进行全外显子组测序未能发现导致孟德尔免疫性疾病的致病性变异。每年在夏季中断免疫球蛋白替代治疗的评估未能显示出在接受 RTX 治疗 7 年和 10 年后,内源性免疫球蛋白产生或类别转换记忆 B 细胞的正常数量恢复。尽管导致利妥昔单抗治疗后持续性低丙种球蛋白血症的因素(如有必要)尚不清楚,但在治疗前进行全面的免疫学检查和长期随访是评估长期并发症的必要条件,尤其是在儿童中。