Biomedical Imaging Science Department, Leeds Institute of Cardiovascular and Metabolic Medicine, University of Leeds, Leeds Teaching Hospitals NHS Trust, Leeds, UK.
Institute for Biomedical Engineering, University and ETH Zurich, Zurich, Switzerland.
J Magn Reson Imaging. 2022 Oct;56(4):1171-1181. doi: 10.1002/jmri.28063. Epub 2022 Jan 12.
Intramyocardial hemorrhage (IMH) following ST-elevation myocardial infarction (STEMI) is associated with poor prognosis. In cardiac magnetic resonance (MR), T2* mapping is the reference standard for detecting IMH while cardiac diffusion tensor imaging (cDTI) can characterize myocardial architecture via fractional anisotropy (FA) and mean diffusivity (MD) of water molecules. The value of cDTI in the detection of IMH is not currently known.
cDTI can detect IMH post-STEMI.
Prospective.
A total of 50 patients (20% female) scanned at 1-week (V1) and 3-month (V2) post-STEMI.
FIELD STRENGTH/SEQUENCE: A 3.0 T; inversion-recovery T1-weighted-imaging, multigradient-echo T2* mapping, spin-echo cDTI.
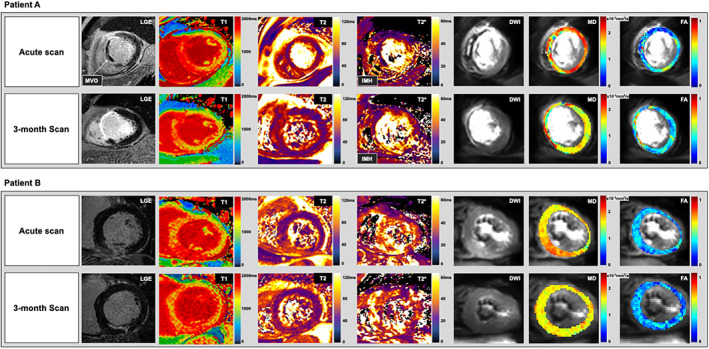
T2* maps were analyzed to detect IMH (defined as areas with T2* < 20 msec within areas of infarction). cDTI images were co-registered to produce averaged diffusion-weighted-images (DWIs), MD, and FA maps; hypointense areas were manually planimetered for IMH quantification.
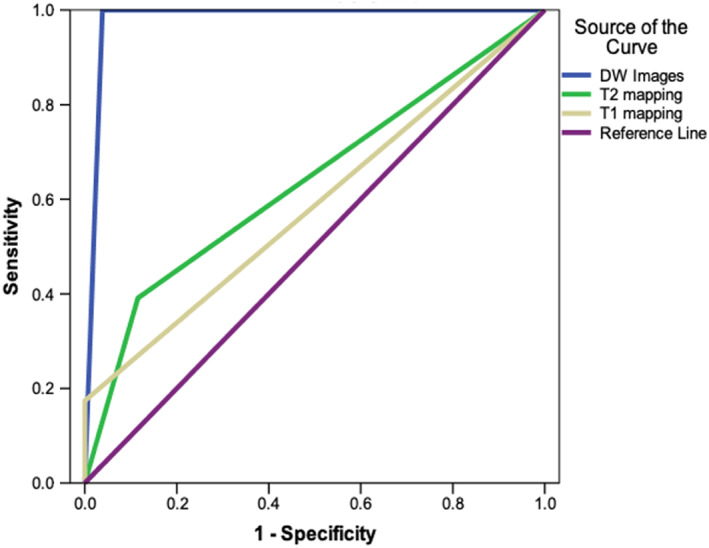
On averaged DWI, the presence of hypointense signal in areas matching IMH on T2* maps constituted to true-positive detection of iron. Independent samples t-tests were used to compare regional cDTI values. Results were considered statistically significant at P ≤ 0.05.
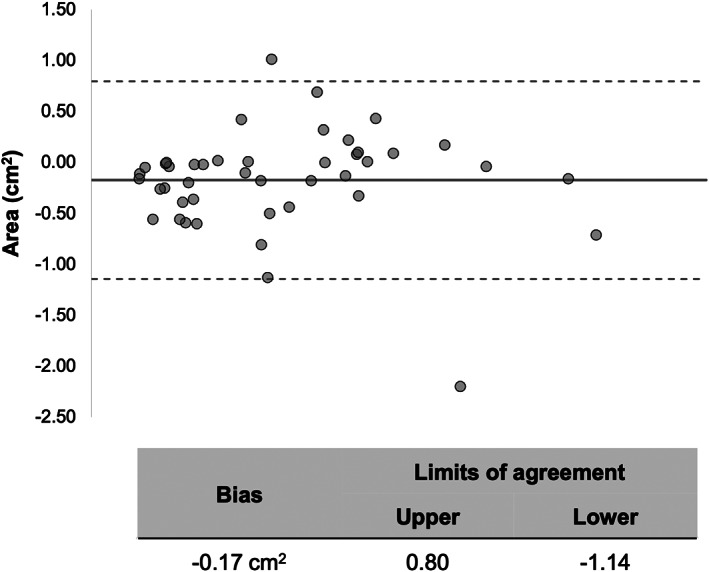
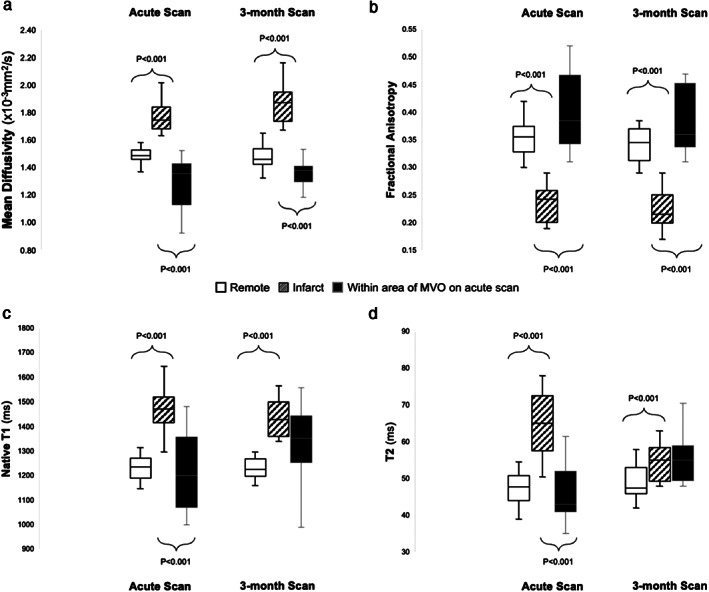
At V1, 24 patients had IMH on T2*. On averaged DWI, all 24 patients had hypointense signal in matching areas. IMH size derived using averaged-DWI was nonsignificantly greater than from T2* (2.0 ± 1.0 cm vs 1.89 ± 0.96 cm , P = 0.69). Compared to surrounding infarcted myocardium, MD was significantly reduced (1.29 ± 0.20 × 10 mm /sec vs 1.75 ± 0.16 × 10 mm /sec) and FA was significantly increased (0.40 ± 0.07 vs 0.23 ± 0.03) within areas of IMH. By V2, all 24 patients with acute IMH continued to have hypointense signals on averaged-DWI in the affected area. T2* detected IMH in 96% of these patients. Overall, averaged-DWI had 100% sensitivity and 96% specificity for the detection of IMH.
This study demonstrates that the parameters MD and FA are susceptible to the paramagnetic properties of iron, enabling cDTI to detect IMH.
1 TECHNICAL EFFICACY: Stage 2.
ST 段抬高型心肌梗死(STEMI)后发生的心肌内出血(IMH)与预后不良有关。在心脏磁共振(CMR)中,T2* 映射是检测 IMH 的参考标准,而心脏扩散张量成像(cDTI)可以通过水分子的分数各向异性(FA)和平均扩散系数(MD)来描述心肌结构。cDTI 在检测 IMH 中的价值目前尚不清楚。
cDTI 可以检测 STEMI 后的 IMH。
前瞻性。
共 50 名患者(20%为女性),在 STEMI 后 1 周(V1)和 3 个月(V2)进行扫描。
磁场强度/序列:3.0T;反转恢复 T1 加权成像、多梯度回波 T2* 映射、自旋回波 cDTI。
分析 T2* 图谱以检测 IMH(定义为在梗死区域内 T2* < 20msec 的区域)。将 cDTI 图像配准以生成平均扩散加权图像(DWI)、MD 和 FA 图;手动描绘低信号区域以进行 IMH 定量。
在平均 DWI 上,在与 T2* 图谱上 IMH 匹配的区域中出现低信号构成铁的真阳性检测。使用独立样本 t 检验比较区域 cDTI 值。结果 P ≤ 0.05 时认为具有统计学意义。
在 V1 时,24 名患者的 T2* 上有 IMH。在平均 DWI 上,所有 24 名患者在匹配区域均有低信号。使用平均 DWI 得出的 IMH 大小与 T2* 无显著差异(2.0 ± 1.0cm 与 1.89 ± 0.96cm,P=0.69)。与周围梗死心肌相比,MD 明显降低(1.29 ± 0.20×10mm/sec 与 1.75 ± 0.16×10mm/sec),FA 明显增加(0.40 ± 0.07 与 0.23 ± 0.03)在 IMH 区域内。到 V2 时,所有 24 名急性 IMH 患者在受影响区域的平均 DWI 上继续有低信号。T2* 在这些患者中的 96%中检测到 IMH。总的来说,平均 DWI 对 IMH 的检测具有 100%的敏感性和 96%的特异性。
本研究表明,参数 MD 和 FA 易受铁的顺磁性特性的影响,使 cDTI 能够检测 IMH。
1 技术功效:2 级。