Clinical Research Unit, Tata Translational Cancer Research Centre, Tata Medical Centre, 14 MAR (E-W), New Town, Kolkata, West Bengal, 700160, India.
Department of Pediatric Oncology, Tata Memorial Centre, Tata Memorial Hospital, Mumbai, Maharashtra, 400012, India.
Trials. 2022 Jan 31;23(1):102. doi: 10.1186/s13063-022-06033-1.
In the west, survival following treatment of childhood acute lymphoblastic leukaemia (ALL) approaches 90%. Outcomes in India do not exceed 70%. To address this disparity, the Indian Collaborative Childhood Leukaemia group (ICiCLe) developed in 2013 a contemporary treatment protocol for uniform risk-stratified management of first presentation ALL based on cytogenetics and minimal residual disease levels (MRD). A multicentre randomised clinical trial opened in 2016 (ICiCLe-ALL-14) and examines the benefit of randomised interventions to decrease toxicity and improve outcomes.
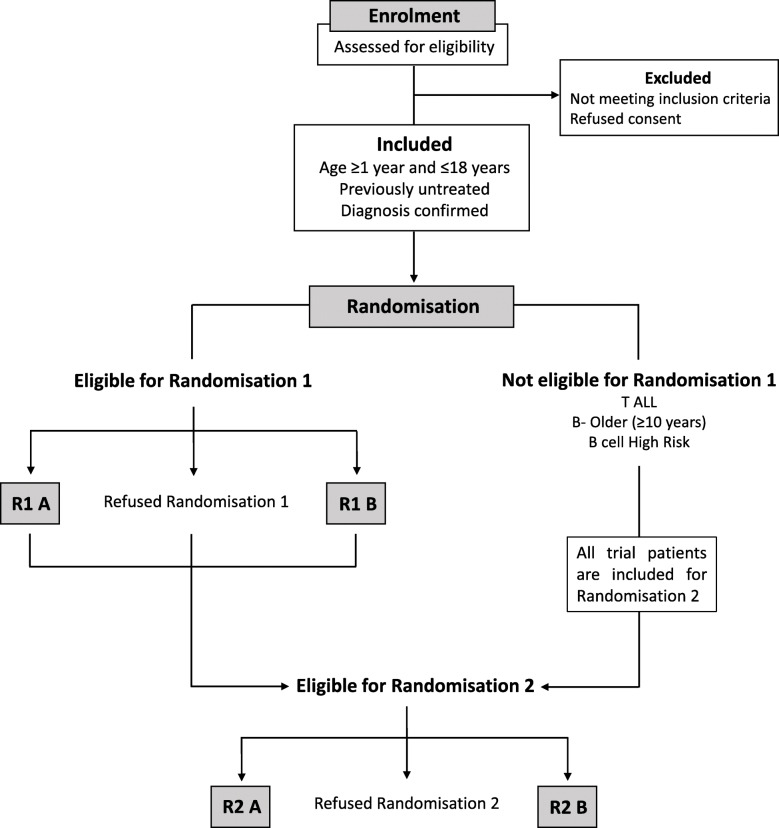
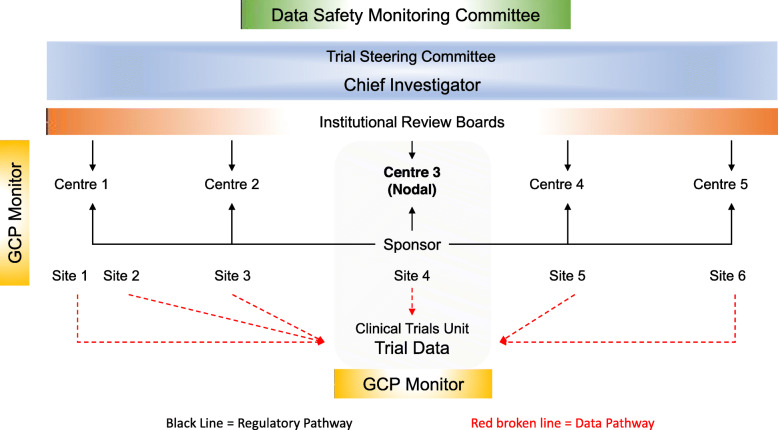
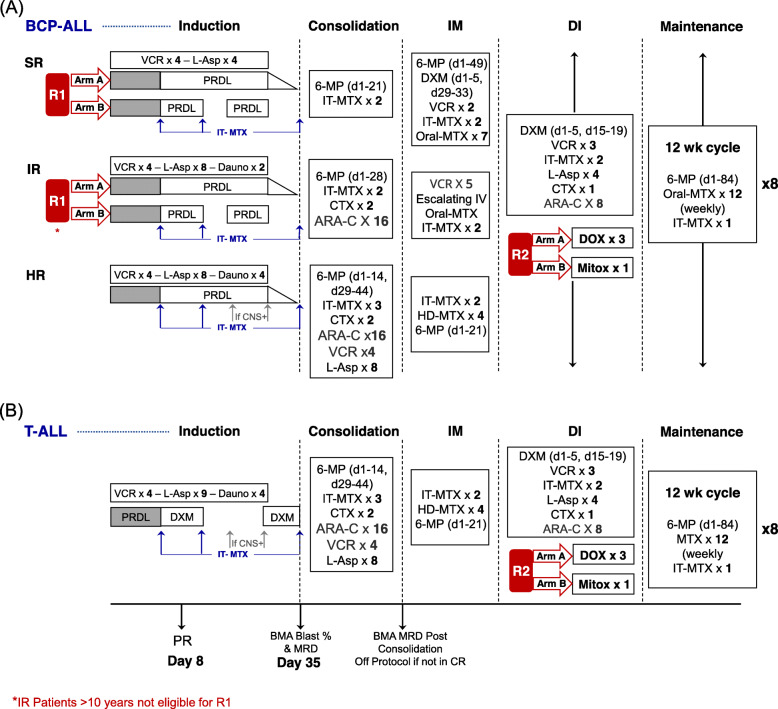
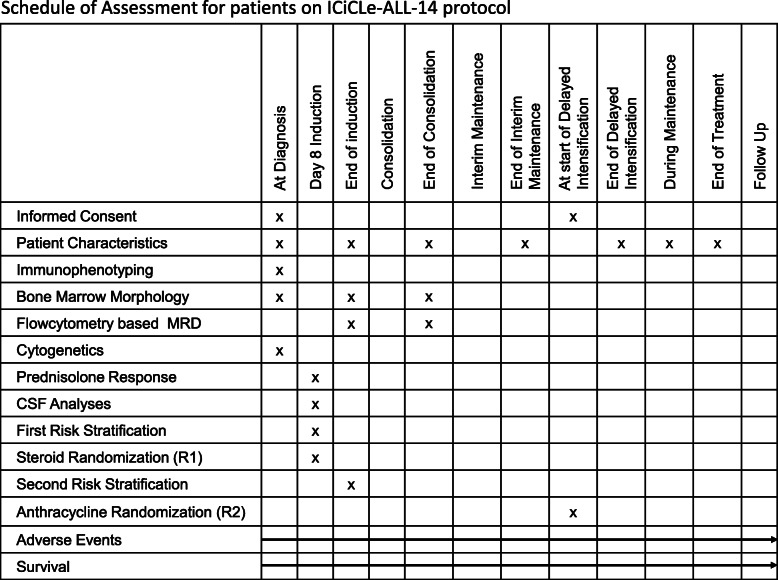
Patients 1-18 years with newly diagnosed ALL are categorised into four risk groups based on presentation features, tumour genetics and treatment response. Standard risk includes young (< 10 years) B cell precursor ALL (BCP-ALL) patients with low presentation leucocyte count (< 50 × 10/L) and no high-risk features. Intermediate risk includes BCP-ALL patients with no high-risk features but are older and have high presentation leucocyte counts and/or bulky disease. High risk includes BCP-ALL patients with any high-risk feature, including high-risk genetics, central nervous system leukaemia, poor prednisolone response at treatment day 8 and high MRD (≥ 0·01%) at the end of induction. Patients with T-lineage ALL constitute the fourth risk group. All patients receive four intensive treatment blocks (induction, consolidation, interim maintenance, delayed intensification) followed by 96 weeks of maintenance. Treatment intensity varies by risk group. Clinical data management is based on a web-based remote data capture system. The first randomisation examines the toxicity impact of a shorter induction schedule of prednisolone (3 vs 5 weeks) in young non-high-risk BCP-ALL. The second randomisation examines the survival benefit of substituting doxorubicin with mitoxantrone in delayed intensification for all patients. Primary outcome measures include event-free survival (overall, by risk groups), sepsis rates in induction (first randomisation) and event-free survival rates following second randomisation.
ICiCLe-ALL-14 is the first multicentre randomised childhood cancer clinical trial in India. The pre-trial phase allowed standardisation of risk-stratification diagnostics and established the feasibility of collaborative practice, uniform treatment, patient enrolment and data capture. Pre-trial observations confirm the impact of risk-stratified therapy in reducing treatment-related deaths and costs. Uniform practice across centres allows patients to access care locally, potentially decreasing financial hardship and dislocation.
Clinical Trials Registry-India (CTRI) CTRI/2015/12/006434 . Registered on 11 December 2015.
在西方,儿童急性淋巴细胞白血病(ALL)治疗后的生存率接近 90%。而印度的生存率不超过 70%。为了解决这一差距,印度协作儿童白血病组(ICiCLe)于 2013 年制定了一种基于细胞遗传学和微小残留病(MRD)水平的当代治疗方案,用于对首次表现 ALL 进行统一的风险分层管理。一项多中心随机临床试验于 2016 年(ICiCLe-ALL-14)开放,并检查了随机干预降低毒性和改善结果的益处。
新诊断为 ALL 的 1-18 岁患者根据临床表现、肿瘤遗传学和治疗反应分为四个风险组。标准风险包括年轻(<10 岁)B 细胞前体 ALL(BCP-ALL)患者,其白细胞计数较低(<50×10/L)且无高危特征。中危组包括无高危特征但年龄较大、白细胞计数较高且/或有肿块的 BCP-ALL 患者。高危组包括具有任何高危特征的 BCP-ALL 患者,包括高危遗传学、中枢神经系统白血病、治疗第 8 天泼尼松预治疗反应差和诱导结束时 MRD 较高(≥0.01%)。T 细胞系 ALL 患者构成第四组。所有患者接受四个强化治疗阶段(诱导、巩固、中期维持、延迟强化),然后进行 96 周的维持治疗。治疗强度根据风险组而异。临床数据管理基于基于网络的远程数据采集系统。第一次随机化检查了年轻非高危 BCP-ALL 患者泼尼松诱导期较短(3 周与 5 周)的毒性影响。第二次随机化检查了在所有患者的延迟强化治疗中用米托蒽醌替代多柔比星对生存获益的影响。主要终点包括无事件生存(总体、按风险组)、诱导期中的败血症发生率(第一次随机化)和第二次随机化后的无事件生存率。
ICiCLe-ALL-14 是印度首例多中心儿童癌症临床试验。试验前阶段允许风险分层诊断的标准化,并建立了协作实践、统一治疗、患者入组和数据采集的可行性。试验前观察结果证实了风险分层治疗在降低治疗相关死亡和成本方面的作用。各中心的统一实践使患者能够在当地获得治疗,可能会减轻经济困难和流离失所的问题。
印度临床试验注册处(CTRI)CTRI/2015/12/006434。于 2015 年 12 月 11 日注册。