Department of Neurological Sciences, University of Vermont Medical Center and Robert Larner, MD College of Medicine, University of Vermont, Burlington, VT, USA.
General Clinical Research Center, University of Vermont Medical Center and Robert Larner, MD College of Medicine, University of Vermont, Burlington, VT, USA.
Am J Clin Nutr. 2022 May 1;115(5):1378-1392. doi: 10.1093/ajcn/nqac016.
Motor neuron degeneration and malnutrition alter body composition in amyotrophic lateral sclerosis (ALS). Resulting losses of weight, fat mass (FM), and fat-free mass (FFM) shorten survival. Nutritional management relies on body weight or BMI; neither reliably indicates malnutrition nor differentiates body compartments.
We aimed to 1) develop an equation to compute FM and FFM using clinical data, validated against DXA; and 2) examine the effect of computed FM and FFM on disease course and survival.
We studied 364 ALS patients from 3 cohorts. In Cohort #1 we used logistic regression on clinical and demographic data to create an equation (test cohort). In Cohort #2 we validated FM and FFM computed using this equation against DXA (validation cohort). In Cohort #3, we examined the effect of computed body composition on disease course and survival.
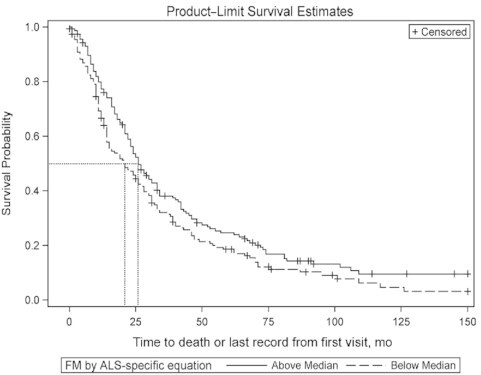
In Cohort #1 (n = 29) the model incorporated sex, age, BMI, and bulbar-onset to create an equation to estimate body fat: % body fat = 1.73 - [19.80gender (1 if male or 0 if female)] + [0.25weight (kg)] + [0.95BMI (kg/m2)] - (5.201 if bulbar-onset or *0 if limb-onset). In Cohort #2 (n = 104), body composition using this equation, compared to other published equations, showed the least variance from DXA values. In Cohort #3 (n = 314), loss of body composition over 6 mo was greater in males. Adjusted survival was predicted by low baseline FM (HR: 1.39; 95% CI: 1.07, 1.80), and loss of FM (HR: 1.87; 95% CI: 1.30, 2.69) and FFM (HR: 1.73; 95% CI: 1.20, 2.49) over 6 mo.
Our equation broadens the traditional nutritional evaluation in clinics and reliably estimates body composition. Measuring body composition could target FM as a focus for nutritional management to ensure adequate energy intake and complement measures, such as the ALS functional rating scale-revised score and forced vital capacity, currently used.
运动神经元变性和营养不良会改变肌萎缩侧索硬化症(ALS)患者的身体成分。体重、脂肪量(FM)和去脂体重(FFM)的减少会缩短生存期。营养管理依赖于体重或 BMI;两者均不能可靠地指示营养不良,也不能区分身体部位。
我们旨在 1)开发一种使用临床数据计算 FM 和 FFM 的方程,并通过 DXA 进行验证;2)研究计算得出的 FM 和 FFM 对疾病进程和生存的影响。
我们研究了来自 3 个队列的 364 名 ALS 患者。在队列 #1 中,我们使用逻辑回归对临床和人口统计学数据进行分析,创建了一个方程(测试队列)。在队列 #2 中,我们通过 DXA 验证了使用该方程计算得出的 FM 和 FFM(验证队列)。在队列 #3 中,我们研究了计算得出的身体成分对疾病进程和生存的影响。
在队列 #1(n=29)中,该模型纳入了性别、年龄、BMI 和延髓发病,以创建一个估算体脂的方程:体脂%=1.73-(19.80性别(男性为 1,女性为 0))+(0.25体重(kg))+(0.95BMI(kg/m2))-(5.20延髓发病或 0*肢体发病)。在队列 #2(n=104)中,与其他已发表的方程相比,使用该方程计算得出的身体成分与 DXA 值的差异最小。在队列 #3(n=314)中,男性在 6 个月内身体成分的丢失量更大。调整后的生存预测因素为基线时低 FM(HR:1.39;95%CI:1.07,1.80)、6 个月内 FM (HR:1.87;95%CI:1.30,2.69)和 FFM(HR:1.73;95%CI:1.20,2.49)的丢失。
我们的方程扩展了临床传统的营养评估,并能可靠地估算身体成分。测量身体成分可以将 FM 作为营养管理的重点,以确保摄入足够的能量,并补充目前使用的 ALS 功能评定量表修订版评分和用力肺活量等措施。