Department of Cardiovascular Medicine and Director of Mountain Medicine, Research, and Survey Division, Hokkaido Ono Memorial Hospital, Sapporo, Hokkaido, Japan
Department of Internal Medicine, Nihon University School of Medicine, Tokyo, Japan.
BMJ Open. 2022 Feb 3;12(2):e053935. doi: 10.1136/bmjopen-2021-053935.
This study aimed to describe the cause of death and characteristics at the prehospital setting associated with care and rescue processes of non-survivors rescued in the mountain of Japan.
Retrospective analysis.
Prehospital setting of mountain searches and rescues in Japan. A total of 10 prefectural police headquarters with >10 cases of mountain death from 2011 to 2015.
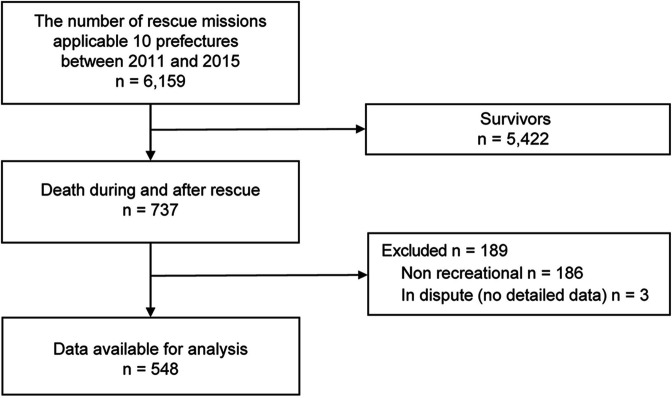
Data were generated from the existing records. Of the total 6159 rescued subjects, 548 mountain deaths were caused by recreational activities.
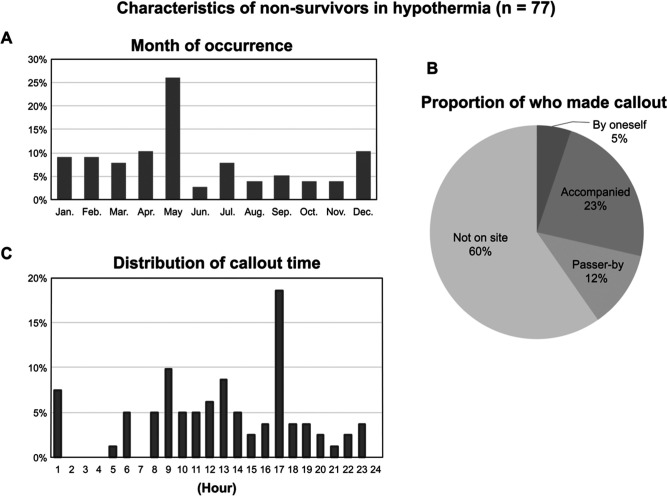
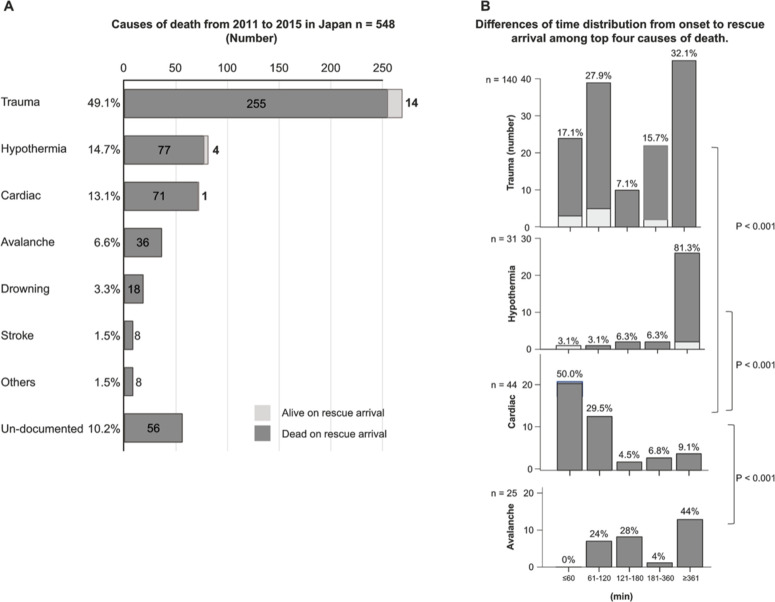
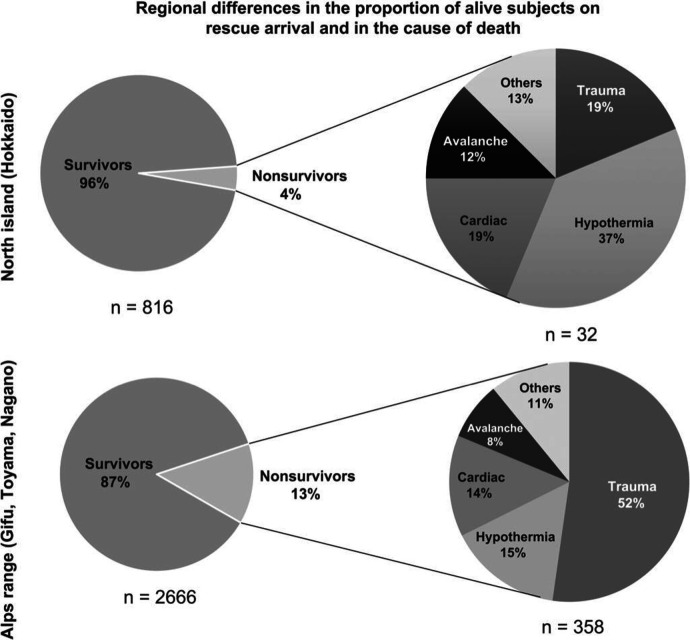
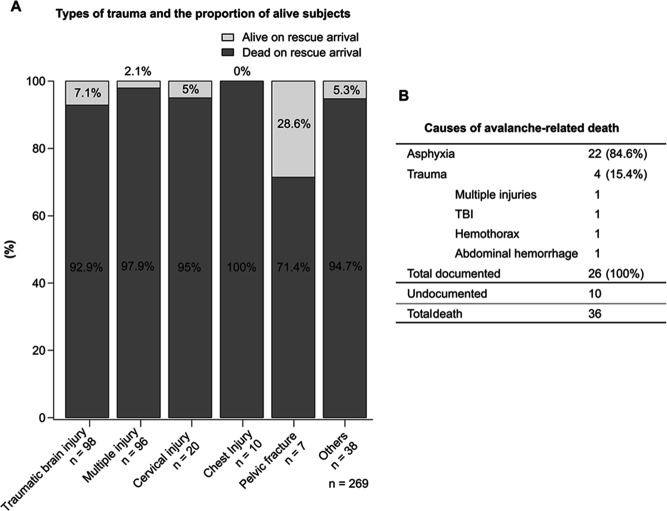
Among the 548 mountain deaths, 83% were men, and major causes of death were trauma (49.1%), hypothermia (14.8%), cardiac death (13.1%) and avalanche-related death (6.6%). The alive rate at rescue team arrival in all non-survivors was 3.5%, with 1, 4 and 14 cases of cardiac, hypothermia and trauma, respectively. Cardiac deaths occurred in 93.1% (67/72) of men and individuals aged >41 years, and 88.7% (63/71) were found on mountain trails. In hypothermia, callouts were made between 17:00 and 6:00 at 49% (40/81) and by persons not on-site in 59.7% (46/77). People with >6 hours in trauma or >1 hour in cardiac death already died on rescue team arrival, but some with hypothermia after 6 hours were alive.
This study is one of the first large-scale retrospective analyses of prehospital non-survivors in mountain emergencies. The alive rate at rescue arrival in all mountain deaths was only 3.5%. These data showed that the circumstances related to onset and the process until the rescue team arrives have different characteristics, depending on the cause of death. Survival may be enhanced by targeting better use of the time before rescue team arrival and by providing further education, particularly mountain rescue-related medical problems to rescuers including bystanders.
本研究旨在描述日本山区搜救过程中与医疗和救援相关的院前死亡原因和特征。
回顾性分析。
日本山区搜救的院前环境。2011 年至 2015 年期间,共有 10 个县警察总部报告了超过 10 例与山地死亡相关的案例。
数据来源于现有记录。在总共 6159 名获救者中,548 人因娱乐活动而死亡。
在 548 例山地死亡中,83%为男性,主要死因包括创伤(49.1%)、体温过低(14.8%)、心源性死亡(13.1%)和雪崩相关死亡(6.6%)。在所有非幸存者中,救援队伍到达时的存活率为 3.5%,分别有 1 例、4 例和 14 例心源性、体温过低和创伤患者。心源性死亡发生在 93.1%(67/72)的男性和年龄>41 岁的个体中,88.7%(63/71)发生在山路。体温过低时,49%(40/81)的呼救发生在 17:00 至 6:00 之间,59.7%(46/77)的呼救来自非现场人员。创伤患者在救援队伍到达时已经死亡超过 6 小时,心源性死亡患者已经死亡超过 1 小时,但体温过低患者在 6 小时后仍有存活。
这是首次对山区紧急情况中院前非幸存者进行的大规模回顾性分析之一。在所有山地死亡中,救援队伍到达时的存活率仅为 3.5%。这些数据表明,与发病相关的情况和直到救援队伍到达的过程具有不同的特征,具体取决于死因。通过更好地利用救援队伍到达之前的时间,并向救援人员(包括旁观者)提供进一步的教育,特别是与山地救援相关的医疗问题,可能会提高生存率。