Jockey Club School of Public Health and Primary Care, The Chinese University of Hong Kong, Hong Kong Special Administrative Region, Hong Kong, China.
Centre for Health Systems & Policy Research, The Chinese University of Hong Kong, Hong Kong Special Administrative Region, Hong Kong, China.
JAMA Netw Open. 2022 Feb 1;5(2):e2145685. doi: 10.1001/jamanetworkopen.2021.45685.
Hong Kong's internal resource allocation system for public inpatient care changed from a global budget system to one based on diagnosis-related groups (DRGs) in 2009 and returned to a global budget system in 2012. Changes in patient and hospital outcomes associated with moving from a DRG-based system to a global budget system for inpatient care have rarely been evaluated.
To examine associations between the introduction and discontinuation of DRGs and changes in length of stay, volume of care, in-hospital mortality rates, and emergency readmission rates in the inpatient population in acute care hospitals overall, stratified by age group, and across 5 medical conditions.
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study included data from patients aged 45 years or older who were hospitalized in public acute care settings in Hong Kong before the introduction (April 2006 to March 2009), during implementation (April 2009 to March 2012), and after discontinuation (April 2012 to November 2014) of the DRG scheme. Data analysis was conducted from January to June 2021.
Public hospitals transitioned from a global budget payment system to a DRG-based system in April 2009 and returned to a global budget system in April 2014.
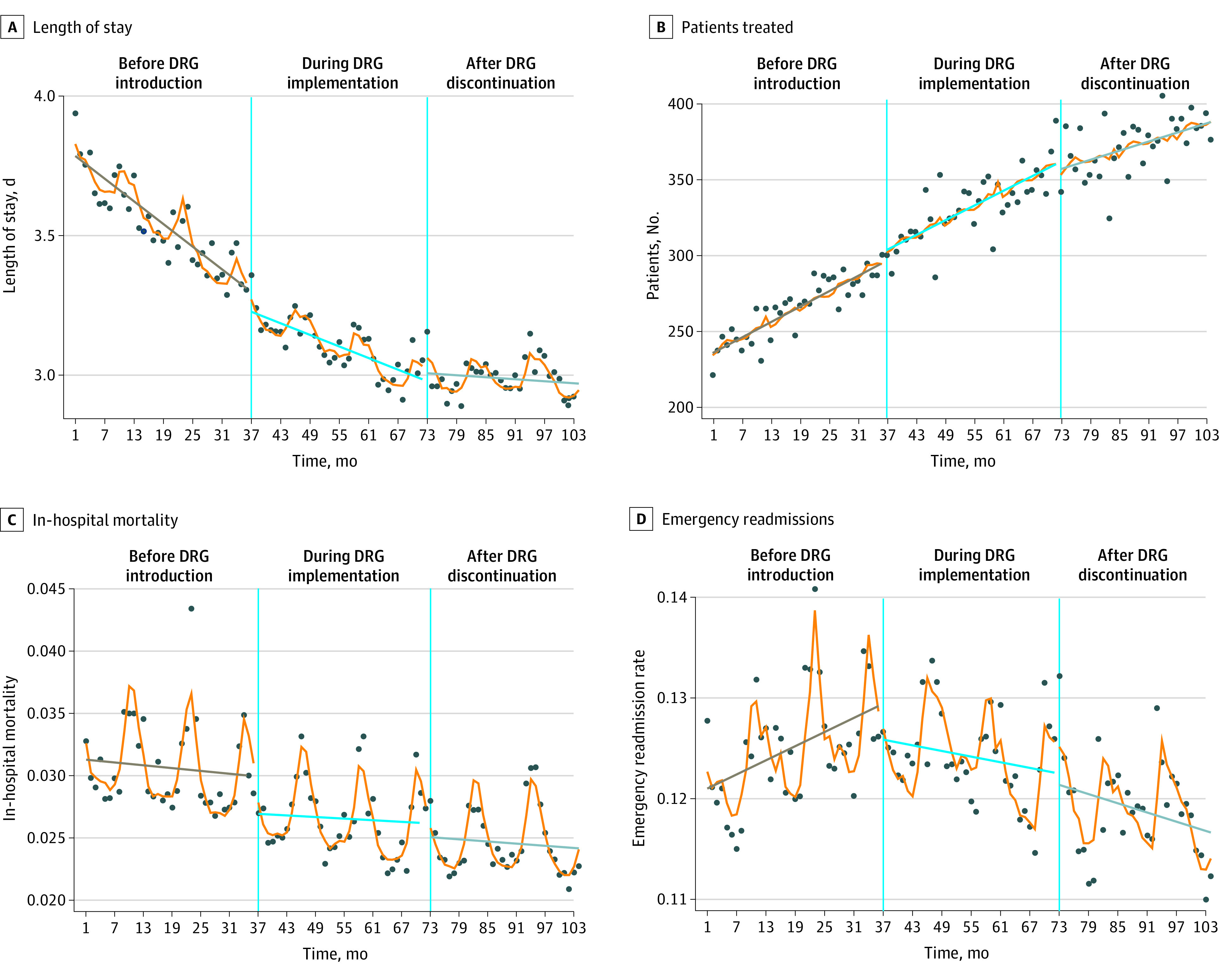
The main outcome was the association of use of DRGs with patient-level length of stay, in-hospital mortality rate, 1-month emergency readmission rate, and population-level number of admissions per month. An interrupted time series design was used to estimate changes in the level and slope of outcome variables after introduction and discontinuation of DRGs, accounting for pretrends.
This study included 7 604 390 patient episodes. Overall, the mean (SD) age of patients was 68.97 (13.20) years, and 52.17% were male. The introduction of DRGs was associated with a 1.77% (95% CI, 1.23%-2.32%) decrease in the mean length of stay, a 2.90% (95% CI, 2.52%-3.28%) increase in the number of patients admitted, a 4.12% (95% CI, 1.89%-6.35%) reduction in in-hospital mortality, and a 2.37% (95% CI, 1.28%-3.46%) decrease in emergency readmissions. Discontinuation of the DRG scheme was associated with a 0.93% (95% CI, 0.42%-1.44%) increase in the mean length of stay and a 1.82% (95% CI, 1.47%-2.17%) reduction in the number of patients treated after adjusting for covariates; no statistically significant change was observed in in-hospital mortality (-0.14%; 95% CI, -2.29% to 2.01%) or emergency readmission rate (-0.29%; 95% CI, -1.30% to 0.71%).
In this cross-sectional study, the introduction of DRGs was associated with shorter lengths of stay and increased hospital volume, and discontinuation was associated with longer lengths of stay and decreased hospital volume. In-hospital mortality and emergency readmission rates did not significantly change after discontinuation of DRGs.
香港的公共住院患者内部资源分配系统于 2009 年从全球预算系统改为基于诊断相关组(DRG)的系统,并于 2012 年重新采用全球预算系统。有关从基于 DRG 的系统转向住院患者的全球预算系统后患者和医院结果变化的研究很少。
评估在全港急症医院的住院人群中,引入和停止使用 DRG 对整体、按年龄组和 5 种医疗条件分类的住院时间、护理量、院内死亡率和急诊再入院率的影响。
设计、地点和参与者:这项回顾性研究包括在香港公立医院接受治疗的年龄在 45 岁及以上的患者数据,患者在 DRG 方案引入(2006 年 4 月至 2009 年 3 月)、实施(2009 年 4 月至 2012 年 3 月)和停止使用(2012 年 4 月至 2014 年 11 月)期间住院的情况。数据分析于 2021 年 1 月至 6 月进行。
公立医院于 2009 年 4 月从全球预算支付系统过渡到基于 DRG 的系统,并于 2014 年 4 月重新采用全球预算系统。
主要结果是使用 DRG 与患者的住院时间、院内死亡率、1 个月的急诊再入院率和每月的住院人数之间的关系。采用中断时间序列设计来估计引入和停止使用 DRG 后结局变量的水平和斜率的变化,同时考虑到预先趋势。
这项研究共纳入了 7604390 个患者的病历。总的来说,患者的平均(SD)年龄为 68.97(13.20)岁,52.17%为男性。引入 DRG 与平均住院时间缩短 1.77%(95%CI,1.23%-2.32%)、入院人数增加 2.90%(95%CI,2.52%-3.28%)、院内死亡率降低 4.12%(95%CI,1.89%-6.35%)和急诊再入院率降低 2.37%(95%CI,1.28%-3.46%)有关。停止使用 DRG 方案与平均住院时间增加 0.93%(95%CI,0.42%-1.44%)和接受治疗的患者数量减少 1.82%(95%CI,1.47%-2.17%)有关,经调整协变量后,院内死亡率(-0.14%;95%CI,-2.29%至 2.01%)或急诊再入院率(-0.29%;95%CI,-1.30%至 0.71%)无统计学意义的变化。
在这项回顾性研究中,引入 DRG 与住院时间缩短和医院容量增加有关,而停止使用 DRG 与住院时间延长和医院容量减少有关。停止使用 DRG 后,院内死亡率和急诊再入院率没有显著变化。