National Cancer Registry, Building 6800, Cork Airport Business Park, Cork, Ireland.
BMC Health Serv Res. 2012 Mar 26;12:77. doi: 10.1186/1472-6963-12-77.
The impact of developments in colorectal cancer surgery on length-of-stay (LOS) and re-admission have not been well described. In a population-based analysis, we investigated predictors of LOS and emergency readmission after the initial surgery episode.
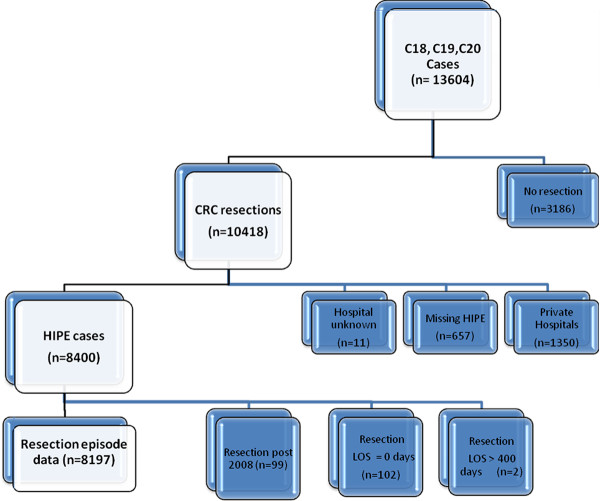
Incident colorectal cancers (ICD-O2: C18-C20), diagnosed 2002-2008, were identified from the National Cancer Registry Ireland, and linked to hospital in-patient episodes. For those who underwent colorectal resection, the associated hospital episode was identified. Factors predicting longer LOS (upper-quartile, > 24 days) for elective and emergency admissions separately, and whether LOS predicted emergency readmission within 28 days of discharge, were investigated using logistic regression.
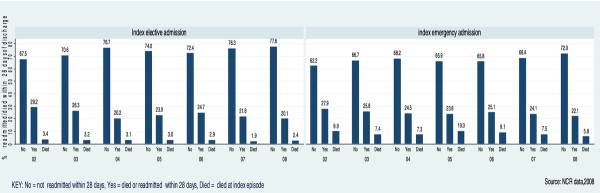
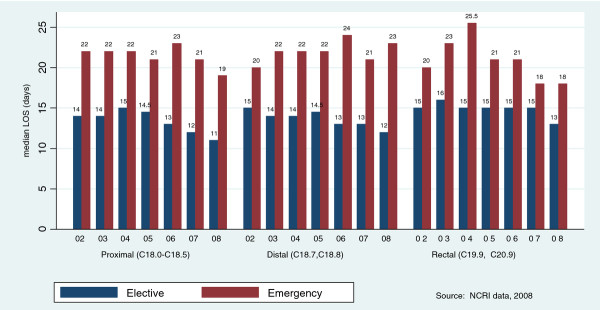
8197 patients underwent resection, 63% (n = 5133) elective and 37% (n = 3063) emergency admissions. Median LOS was 14 days (inter-quartile range (IQR) = 11-20) for elective and 21 (15-33) for emergency admissions. For both emergency and elective admissions, likelihood of longer LOS was significantly higher in patients who were older, had co-morbidities and were unmarried; it was reduced for private patients. For emergency patients only the likelihood of longer LOS was lower for patients admitted to higher-volume hospitals. Longer LOS was associated with increased risk of emergency readmission.
One quarter of patients stay in hospital for at least 25 days following colorectal resection. Over one third of resected patients are emergency admissions and these have a significantly longer median LOS. Patient- and health service-related factors were associated with prolonged LOS. Longer LOS was associated with increased risk of emergency readmission. The cost implications of these findings are significant.
结直肠癌手术的发展对住院时间(LOS)和再入院的影响尚未得到很好的描述。在一项基于人群的分析中,我们调查了初始手术发作后 LOS 和紧急再入院的预测因素。
从爱尔兰国家癌症登记处确定了 2002-2008 年诊断的结直肠癌(ICD-O2:C18-C20)病例,并与医院住院病例相关联。对于接受结直肠切除术的患者,确定了相关的医院住院病例。使用逻辑回归分别调查了择期和紧急入院的较长 LOS(上四分位数,>24 天)的预测因素,以及 LOS 是否预测出院后 28 天内的紧急再入院。
8197 例患者接受了切除术,63%(n=5133)为择期入院,37%(n=3063)为紧急入院。择期和紧急入院的中位 LOS 分别为 14 天(四分位间距(IQR)=11-20)和 21 天(15-33)。对于紧急和择期入院,年龄较大、合并症较多和未婚的患者 LOS 较长的可能性显著较高;私人患者的可能性降低。仅对于紧急患者,住院量较高的医院入院患者的 LOS 较长的可能性较低。较长的 LOS 与紧急再入院的风险增加相关。
四分之一的患者在结直肠切除术后至少住院 25 天。超过三分之一的接受切除术的患者是紧急入院,他们的中位 LOS 明显更长。患者和卫生服务相关因素与 LOS 延长有关。较长的 LOS 与紧急再入院的风险增加相关。这些发现的成本影响是巨大的。