Department of Oncology, Palacký University Medical School and Teaching Hospital, Olomouc, Czech Republic.
Deparment of Clinical Pharmacology, Palacký University Medical School and Teaching Hospital, Olomouc, Czech Republic.
BMC Gastroenterol. 2022 Feb 5;22(1):49. doi: 10.1186/s12876-022-02121-3.
Sunitinib and pazopanib are both oral small molecule multityrosine kinase inhibitors (MTKI) used in the treatment of renal cell carcinoma (RCC). Hepatotoxicity or "liver injury" is the most important adverse effect of pazopanib administration, but little is known about the underlying mechanism. Liver injury may also occur in patients treated with sunitinib, but severe toxicity is extremely rare. Herein we report two new cases of severe liver injury induced by MTKI. Both cases are unique and exceptional. We assessed both cases for drug-induced liver injury (DILI) using the updated score Roussel Uclaf causality assessment method (RUCAM). The literature on potential pathogenic mechanisms and precautionary measures is reviewed.
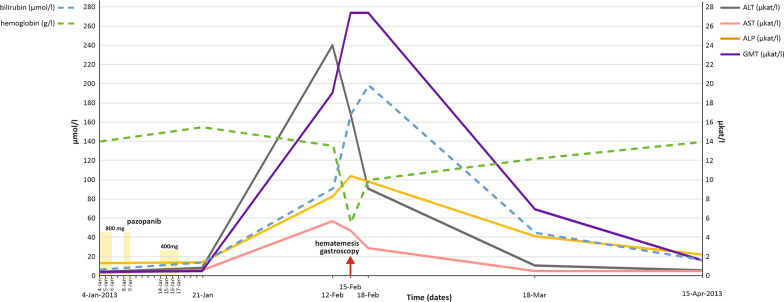
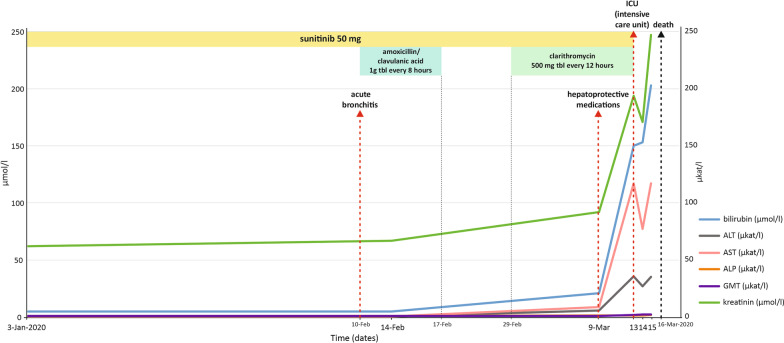
A case of a metastatic RCC (mRCC) patient treated with pazopanib who had manifestation of severe liver injury is presented. These manifestations consisted of grade 4 alanine aminotransferase (ALT) increase and grade 4 hyperbilirubinemia. Alternate causes of acute or chronic liver disease were excluded. The patient gradually recovered from the liver injury and refused any further therapy for mRCC. The patient was diagnosed with acute myeloid leukemia (AML) two years later and eventually succumbed to the disease. The second case describes a mRCC patient treated with sunitinib for 3,5 years and fatal liver failure after 2 weeks of clarithromycin co-medication for acute bronchitis.
Liver injury has been commonly observed in TKI-treated patients with unpredictable course. Management requires regular routine liver enzyme-monitoring and the collaboration of medical oncologist and hepatologist. There is an unmet medical need for a risk stratification and definition of predictive biomarkers to identify potential genetic polymorphisms or other factors associated with TKI-induced liver injury. Any potential unrecommended concomitant therapy has to be avoided.
舒尼替尼和帕唑帕尼均为口服小分子多靶点酪氨酸激酶抑制剂(MTKI),用于治疗肾细胞癌(RCC)。肝毒性或“肝损伤”是帕唑帕尼给药的最重要不良反应,但对于其潜在机制知之甚少。接受舒尼替尼治疗的患者也可能发生肝损伤,但严重毒性极为罕见。在此,我们报告两例由 MTKI 引起的严重肝损伤新病例。这两个病例均是独特和特殊的。我们使用更新的 Roussel Uclaf 因果关系评估方法(RUCAM)对两例病例进行了药物性肝损伤(DILI)评估。回顾了潜在发病机制和预防措施的文献。
报告了一例转移性肾细胞癌(mRCC)患者使用帕唑帕尼治疗后出现严重肝损伤的病例。这些表现包括 4 级丙氨酸转氨酶(ALT)升高和 4 级高胆红素血症。排除了急性或慢性肝病的其他原因。患者的肝损伤逐渐恢复,拒绝接受任何进一步的 mRCC 治疗。两年后,患者被诊断为急性髓系白血病(AML),最终死于该病。第二个病例描述了一名 mRCC 患者,该患者使用舒尼替尼治疗 3.5 年,在因急性支气管炎合用克拉霉素治疗 2 周后发生致命性肝衰竭。
肝损伤在接受 TKI 治疗的患者中很常见,且具有不可预测的病程。管理需要定期进行常规肝酶监测,并需要肿瘤内科医生和肝病学家的协作。需要确定预测生物标志物以识别与 TKI 诱导的肝损伤相关的潜在遗传多态性或其他因素,从而满足未满足的医疗需求。应避免任何潜在的不建议的伴随治疗。