Matuszkiewicz-Rowińska Joanna, Kulicki Paweł, Zebrowski Paweł, Klatko Wiesław, Sokalski Antoni, Niemczyk Stanisław, Wypych-Birecka Magdalena, Małyszko Jolanta
Department of Nephrology, Dialysis and Internal Medicine, Medical University of Warsaw, Warsaw, Poland.
Nephrology Department, Regional Specialty Hospital, Ciechanów, Poland.
Front Med (Lausanne). 2022 Jan 21;8:781191. doi: 10.3389/fmed.2021.781191. eCollection 2021.
The ability of extrarenal tissues to convert 25(OH)D (calcidiol) into 1,25(OH)2D (calcitriol) and dependence of the conversion on substrate levels provide the rationale for supplementing vitamin D in dialysis patients who usually have severe depletion of both: 25(OH)D and 1,25(OH)2D. The primary aim of the study was to compare effects of small doses of cholecalciferol (12,000 IU/week) with frequently used in Europe, small doses of alfacalcidol (1.5 μg/week) or placebo, given for 12 weeks, on serum 1,25(OH)D in hemodialysis patients with 25(OH)D deficiency. Secondary outcomes were changes in serum calcium, phosphate, 25(OH)D, parathyroid hormone (PTH), fibroblast growth factor 23 (FGF23) and sclerostin during the treatment.
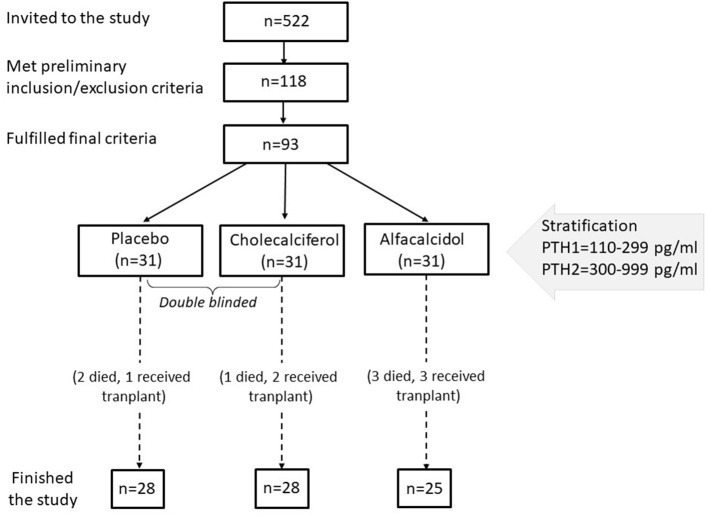
This was a prospective, randomized, partly double-blind (cholecalciferol vs. placebo) study. Out of 522 patients dialyzed in 5 centers in the Mazovian Province, 93 gave informed consent and met the inclusion criteria: any vitamin D metabolites and calcimimetics naïve; no history of liver or intestinal disease; serum 25(OH)D <20 ng/ml, iPTH <1,000 ->110 pg/ml, calcium <10.2, and phosphate <6.8 mg/dl. The subjects were stratified by serum iPTH, then randomized into 3 groups according to the treatment.
To our knowledge, this is the first study comparing head-to-head these drugs in the hemodialysis population. There were no significant differences between the groups at baseline. 81 patients completed the study. Cholecalciferol normalized serum 25(OH)D, with a mean rise from 12.9 ± 6.7 to 31.3 ± 10.1 ng/ml ( < 0.0001). This was accompanied by a marked increase of 1,25(OH)D from 13.8 ± 9.3 to 25.1 ± 14.2 pmol/l ( < 0.0001). A rise in serum 1,25(OH)D was also observed in alfacalcidol treated patients, however much smaller (from 13.5 ± 10.1 to 18.5 ± 11.0 pmol/l; = 0.02). Neither cholecalciferol nor alfacalcidol treatment resulted in significant changes in serum PTH and the remaining parameters.
In most patients, treatment with cholecalciferol in a 12,000 IU/week dose permits safe correction of 25(OH)D deficiency and is more effective than 1.5 μg/week dose of alfacalcidol in rising serum 1,25(OH)D. This, together with a lack of influence on circulating iPTH the usefulness of such small alfacalcidol doses in hemodialysis patients is debatable.
肾外组织将25(OH)D(骨化二醇)转化为1,25(OH)₂D(骨化三醇)的能力以及该转化对底物水平的依赖性,为给通常严重缺乏25(OH)D和1,25(OH)₂D的透析患者补充维生素D提供了理论依据。本研究的主要目的是比较小剂量胆钙化醇(12,000 IU/周)与欧洲常用的小剂量阿法骨化醇(1.5 μg/周)或安慰剂,给予12周,对25(OH)D缺乏的血液透析患者血清1,25(OH)₂D的影响。次要结局是治疗期间血清钙、磷、25(OH)D、甲状旁腺激素(PTH)、成纤维细胞生长因子23(FGF23)和骨硬化蛋白的变化。
这是一项前瞻性、随机、部分双盲(胆钙化醇与安慰剂)研究。在马佐夫舍省5个中心接受透析的522例患者中,93例给予知情同意并符合纳入标准:未使用过任何维生素D代谢物和拟钙剂;无肝脏或肠道疾病史;血清25(OH)D<20 ng/ml,iPTH<1,000~110 pg/ml,钙<10.2,磷<6.8 mg/dl。受试者按血清iPTH分层,然后根据治疗随机分为3组。
据我们所知,这是第一项在血液透析人群中对这些药物进行直接比较的研究。各组在基线时无显著差异。81例患者完成了研究。胆钙化醇使血清25(OH)D恢复正常,平均从12.9±6.7 ng/ml升至31.3±10.1 ng/ml(P<0.0001)。同时,1,25(OH)₂D从13.8±9.3 pmol/l显著升至25.1±14.2 pmol/l(P<0.0001)。阿法骨化醇治疗的患者血清1,25(OH)₂D也有升高,但幅度小得多(从13.5±10.1 pmol/l升至18.5±11.0 pmol/l;P=0.02)。胆钙化醇和阿法骨化醇治疗均未导致血清PTH和其余参数发生显著变化。
在大多数患者中,每周12,000 IU剂量的胆钙化醇治疗可安全纠正25(OH)D缺乏,且在升高血清1,25(OH)₂D方面比每周1.5 μg剂量的阿法骨化醇更有效。鉴于对循环iPTH无影响,如此小剂量的阿法骨化醇在血液透析患者中的实用性值得商榷。