Kunz Wolfgang G, Sporns Peter B, Psychogios Marios N, Fiehler Jens, Chapot René, Dorn Franziska, Grams Astrid, Morotti Andrea, Musolino Patricia, Lee Sarah, Kemmling André, Henkes Hans, Nikoubashman Omid, Wiesmann Martin, Jensen-Kondering Ulf, Möhlenbruch Markus, Schlamann Marc, Marik Wolfgang, Schob Stefan, Wendl Christina, Turowski Bernd, Götz Friedrich, Kaiser Daniel, Dimitriadis Konstantinos, Gersing Alexandra, Liebig Thomas, Ricke Jens, Reidler Paul, Wildgruber Moritz, Mönch Sebastian
Department of Radiology, University Hospital, LMU Munich, Munich, Germany.
Department of Neuroradiology, Clinic for Radiology & Nuclear Medicine, University Hospital Basel, Switzerland.
J Stroke. 2022 Jan;24(1):138-147. doi: 10.5853/jos.2021.01606. Epub 2022 Jan 31.
The Save ChildS Study demonstrated that endovascular thrombectomy (EVT) is a safe treatment option for pediatric stroke patients with large vessel occlusions (LVOs) with high recanalization rates. Our aim was to determine the long-term cost, health consequences and cost-effectiveness of EVT in this patient population.
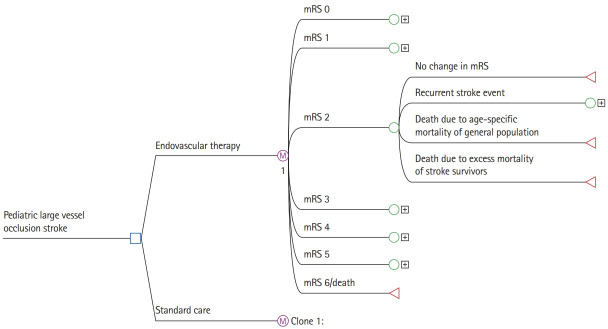
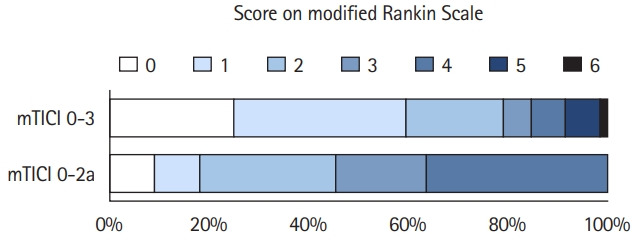
In this retrospective study, a decision-analytic Markov model estimated lifetime costs and quality-adjusted life years (QALYs). Early outcome parameters were based on the entire Save ChildS Study to model the EVT group. As no randomized data exist, the Save ChildS patient subgroup with unsuccessful recanalization was used to model the standard of care group. For modeling of lifetime estimates, pediatric and adult input parameters were obtained from the current literature. The analysis was conducted in a United States setting applying healthcare and societal perspectives. Probabilistic sensitivity analyses were performed. The willingness-to-pay threshold was set to $100,000 per QALY.
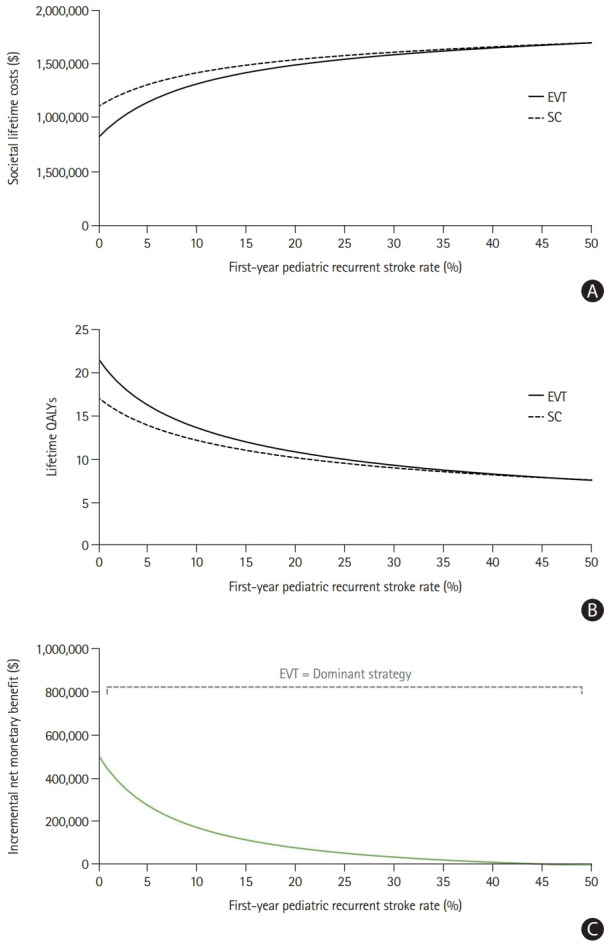
The model.
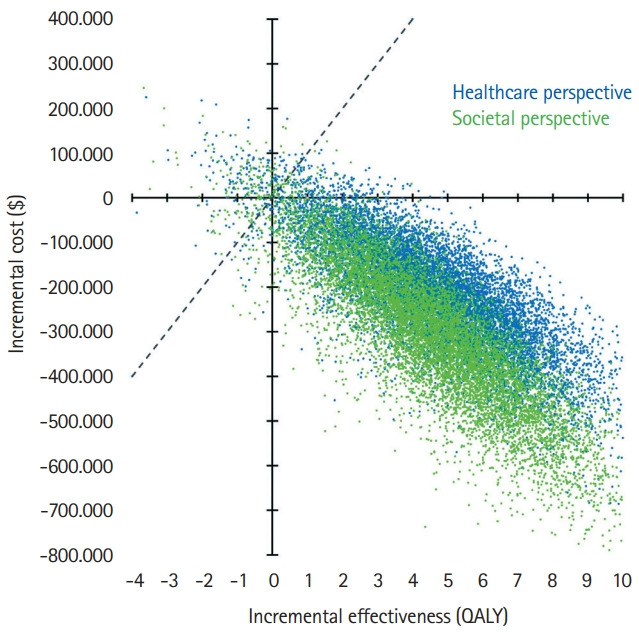
yielded EVT as the dominant (cost-effective as well as cost-saving) strategy for pediatric stroke patients. The incremental effectiveness for the average age of 11.3 years at first stroke in the Save ChildS Study was determined as an additional 4.02 lifetime QALYs, with lifetime cost-savings that amounted to $169,982 from a healthcare perspective and $254,110 when applying a societal perspective. Acceptability rates for EVT were 96.60% and 96.66% for the healthcare and societal perspectives.
EVT for pediatric stroke patients with LVOs resulted in added QALY and reduced lifetime costs. Based on the available data in the Save ChildS Study, EVT is very likely to be a cost-effective treatment strategy for childhood stroke.
儿童卒中挽救研究表明,血管内血栓切除术(EVT)是治疗大血管闭塞(LVO)的儿科卒中患者的一种安全治疗选择,再通率高。我们的目的是确定EVT在该患者群体中的长期成本、健康后果及成本效益。
在这项回顾性研究中,一个决策分析马尔可夫模型估计了终生成本和质量调整生命年(QALY)。早期结局参数基于整个儿童卒中挽救研究来模拟EVT组。由于不存在随机数据,儿童卒中挽救研究中再通失败的患者亚组被用于模拟标准治疗组。对于终生估计的建模,儿科和成人输入参数取自当前文献。分析是在美国环境下从医疗保健和社会角度进行的。进行了概率敏感性分析。支付意愿阈值设定为每QALY 100,000美元。
该模型得出,EVT是儿科卒中患者的主导策略(具有成本效益且节省成本)。在儿童卒中挽救研究中,首次卒中时平均年龄为11.3岁的患者,EVT的增量效益被确定为终生额外增加4.02个QALY,从医疗保健角度看,终生成本节省达169,982美元,从社会角度看为254,110美元。从医疗保健和社会角度看,EVT的可接受率分别为96.60%和96.66%。
对患有LVO的儿科卒中患者进行EVT可增加QALY并降低终生成本。基于儿童卒中挽救研究中的现有数据,EVT很可能是儿童卒中的一种具有成本效益的治疗策略。