Lysosomal Storage Disorders Unit, Institute of Immunity and Transplantation, Royal Free Hospital, Royal Free London NHS Foundation Trust, Rowland Hill Street, London, NW3 2PF, UK.
Department of Haematology, University College London, London, UK.
Orphanet J Rare Dis. 2022 Feb 8;17(1):42. doi: 10.1186/s13023-022-02181-4.
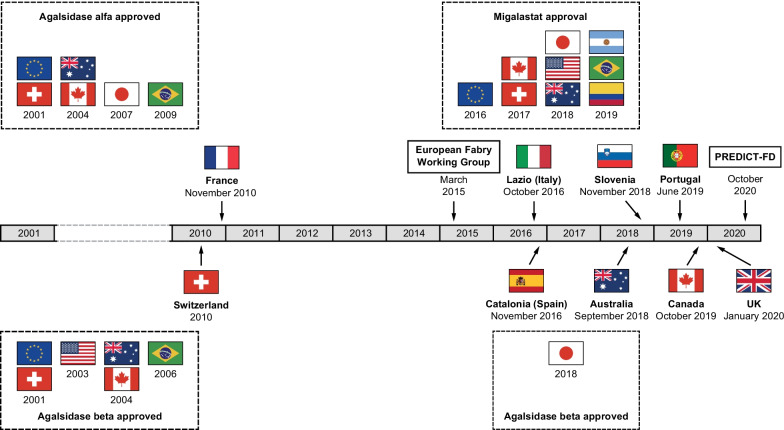
Variable disease progression confounds accurate prognosis in Fabry disease. Evidence supports the long-term benefit of early intervention with disease-specific therapy, but current guidelines recommend treatment initiation based on signs that may present too late to avoid irreversible organ damage. Findings from the 'PRoposing Early Disease Indicators for Clinical Tracking in Fabry Disease' (PREDICT-FD) initiative included expert consensus on 27 early indicators of disease progression in Fabry disease and on drivers of and barriers to treatment initiation in Fabry disease. Here, we compared the PREDICT-FD indicators with guidance from the European Fabry Working Group and various national guidelines to identify differences in signs supporting treatment initiation and how guidelines themselves might affect initiation. Finally, anonymized patient histories were reviewed by PREDICT-FD experts to determine whether PREDICT-FD indicators supported earlier treatment than existing guidance.
Current guidelines generally aligned with PREDICT-FD on indicators of renal involvement, but most lacked specificity regarding cardiac indicators. The prognostic significance of neurological indicators such as white matter lesions (excluded by PREDICT-FD) was questioned in some guidelines and excluded from most. Some PREDICT-FD patient-reported signs (e.g., febrile crises) did not feature elsewhere. Key drivers of treatment initiation in PREDICT-FD were: (A) male sex, young age, and clinical findings (e.g., severe pain, organ involvement), (B) improving clinical outcomes and preventing disease progression, and (C) a family history of Fabry disease (especially if outcomes were severe). All guidelines aligned with (A) and several advocated therapy for asymptomatic male patients. There was scant evidence of (B) in current guidance: for example, no countries mandated ancillary symptomatic therapy, and no guidance advocated familial screening with (C) when diagnosis was confirmed. Barriers were misdiagnosis and a lack of biomarkers to inform timing of treatment. Review of patient histories generally found equal or greater support for treatment initiation with PREDICT-FD indicators than with other guidelines and revealed that the same case and guideline criteria often yielded different treatment recommendations.
Wider adoption of PREDICT-FD indicators at a national level could promote earlier treatment in Fabry disease. Clearer, more concise guidance is needed to harmonize treatment initiation in Fabry disease internationally.
法布里病的疾病进展具有多变性,这使得准确预测预后变得复杂。有证据表明,早期使用特异性疗法进行干预可带来长期获益,但目前的指南建议根据可能出现的体征来启动治疗,而这些体征可能出现得太晚,无法避免器官的不可逆损伤。“法布里病临床跟踪早期疾病指标(PREDICT-FD)”计划的研究结果包括专家对 27 个法布里病疾病进展早期指标的共识,以及对启动法布里病治疗的驱动因素和障碍的共识。在这里,我们将 PREDICT-FD 指标与欧洲法布里工作组以及各种国家指南的指导意见进行了比较,以确定在支持治疗启动的体征以及指南本身如何影响启动治疗方面存在的差异。最后,PREDICT-FD 专家对匿名患者的病史进行了回顾,以确定 PREDICT-FD 指标是否支持比现有指南更早的治疗。
目前的指南在肾脏受累的指标方面与 PREDICT-FD 大致一致,但大多数指南在心脏指标方面缺乏特异性。一些指南质疑了神经指标(如白质病变)的预后意义(PREDICT-FD 将其排除在外),并将其排除在大多数指南之外。PREDICT-FD 的一些患者报告的体征(例如发热性危机)在其他地方没有出现。PREDICT-FD 中启动治疗的关键驱动因素包括:(A)男性、年龄较小和临床发现(如严重疼痛、器官受累);(B)改善临床结局和预防疾病进展;(C)法布里病家族史(尤其是如果结局严重)。所有指南都与(A)一致,并且有几个指南主张对无症状的男性患者进行治疗。目前的指南中几乎没有(B)的证据:例如,没有国家规定进行辅助对症治疗,也没有指南主张在确诊时根据(C)进行家族筛查。障碍包括误诊和缺乏用于确定治疗时机的生物标志物。对患者病史的审查通常发现,使用 PREDICT-FD 指标启动治疗的支持度与其他指南相等或更高,并且发现相同的病例和指南标准通常会产生不同的治疗建议。
在国家层面更广泛地采用 PREDICT-FD 指标可以促进法布里病的早期治疗。需要更明确、更简洁的指南来协调国际上法布里病的治疗启动。