Department of Trauma Surgery, University Medical Center Utrecht, Utrecht, the Netherlands.
Department of Orthopedics and Trauma Surgery, Luzerner Kantonsspital, Spitalstrasse 16, 6000, Lucerne, Switzerland.
Arch Orthop Trauma Surg. 2023 Feb;143(2):887-893. doi: 10.1007/s00402-022-04362-z. Epub 2022 Feb 8.
Multiple rib fractures are associated with significant morbidity and mortality, especially in elderly patients. There is growing interest in surgical stabilization in this subgroup of patients. This systematic review compares conservative treatment to surgical fixation in elderly patients (older than 60 years) with multiple rib fractures. The primary outcome is mortality. Secondary outcomes include hospital and intensive care length of stay (HLOS and ILOS), duration of mechanical ventilation (DMV) and pneumonia rates.
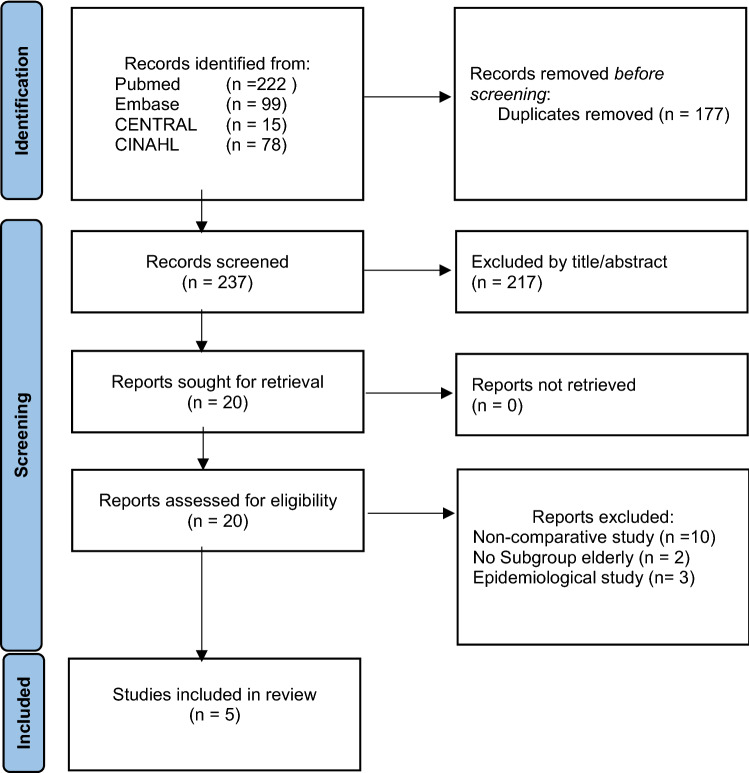
Multiple databases were searched for comparative studies reporting on conservative versus operative treatment for rib fractures in patients older than 60 years. Both observational studies and randomised clinical trials were considered.
Five observational studies (n = 2583) were included. Mortality was lower in operatively treated patients compared to conservative treatment (4% vs. 8%). Pneumonia rate and DMV were similar (5/6% and 5.8/6.5 days) for either treatment modality. Overall ILOS and HLOS of stay were longer in operatively treated patients (6.5 ILOS and 12.7 HLOS vs. 2.7 ILOS and 6.5 ILOS). There were only minimal reports on perioperative complications. Notably, the median number of rib fractures (8.4 vs. 5) and the percentage of flail chest were higher in operatively treated patients (47% vs. 39%).
It remains unknown to what extent conservative and operative treatment contribute individually to reducing morbidity and mortality in the elderly with multiple rib fractures. To date, the quality of evidence is rather low, thus well-performed comparative observational studies or randomised controlled trials considering all confounders are needed to determine whether operative treatment can improve a patient's outcome.
多发性肋骨骨折与较高的发病率和死亡率相关,尤其在老年患者中。人们对这组患者的手术固定越来越感兴趣。本系统评价比较了老年(>60 岁)多发性肋骨骨折患者的保守治疗与手术固定。主要结局是死亡率。次要结局包括住院时间和 ICU 住院时间(HLOS 和 ILOS)、机械通气时间(DMV)和肺炎发生率。
检索了多个数据库中比较 60 岁以上患者保守与手术治疗肋骨骨折的对照研究。纳入了观察性研究和随机临床试验。
共纳入 5 项观察性研究(n=2583)。与保守治疗相比,手术治疗患者的死亡率较低(4%比 8%)。两种治疗方式的肺炎发生率和 DMV 相似(5/6%和 5.8/6.5 天)。手术治疗患者的总 ICU 住院时间和总住院时间较长(6.5 天和 12.7 天比 2.7 天和 6.5 天)。手术治疗患者的肋骨骨折中位数(8.4 比 5)和连枷胸百分比(47%比 39%)更高,但仅有很少的报告涉及围手术期并发症。
目前尚不清楚保守治疗和手术治疗在多大程度上可以分别降低老年多发性肋骨骨折患者的发病率和死亡率。迄今为止,证据质量较低,因此需要进行设计良好的比较观察性研究或随机对照试验,以考虑所有混杂因素,来确定手术治疗是否可以改善患者的预后。