Department of Pathology, University of California San Francisco (UCSF), San Francisco, CA, USA.
Robert J. Tomsich Institute of Pathology and Laboratory Medicine, Cleveland Clinic, Cleveland, OH, USA.
Mod Pathol. 2022 Aug;35(8):1092-1100. doi: 10.1038/s41379-022-01009-7. Epub 2022 Feb 10.
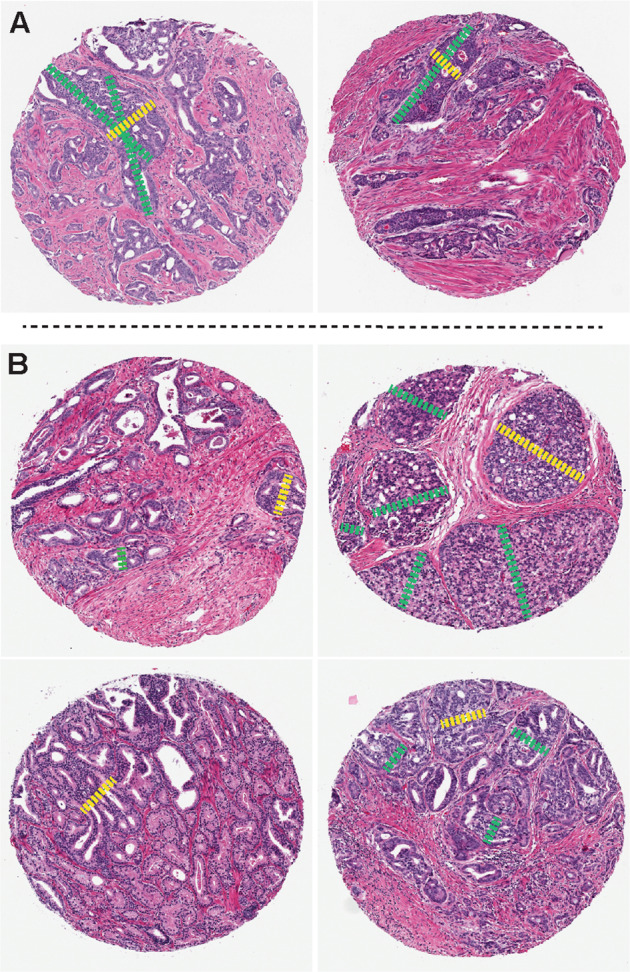
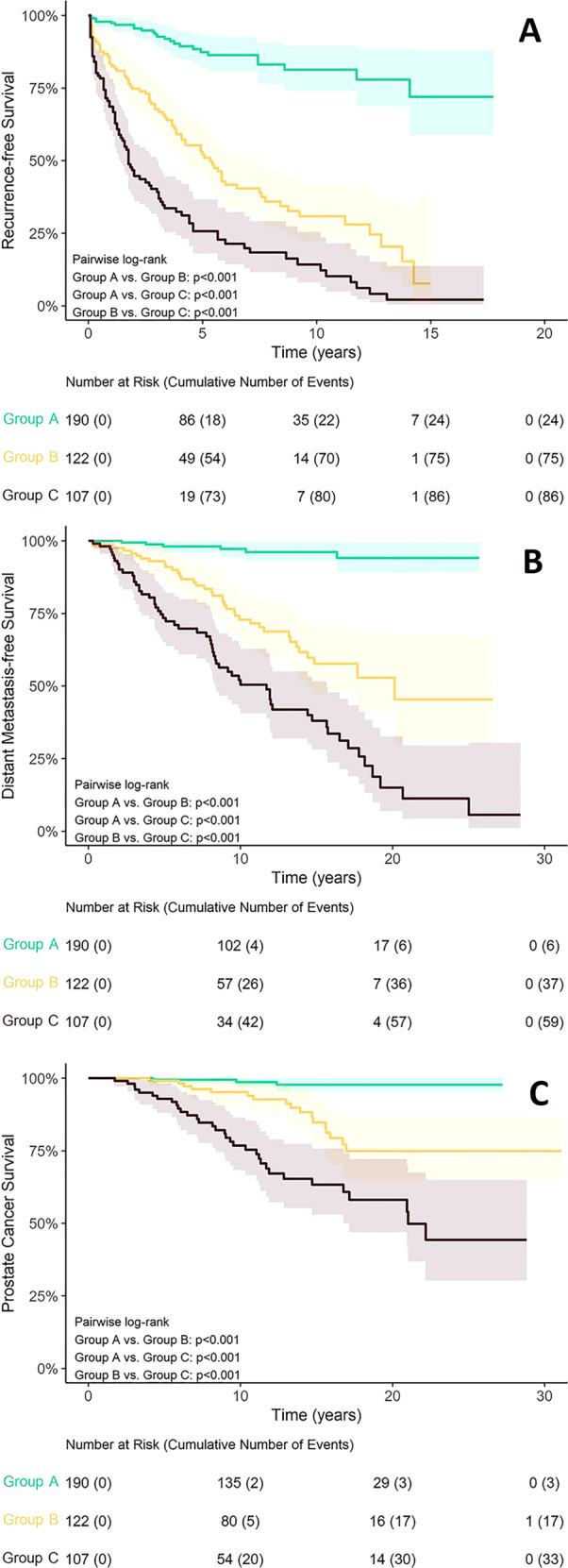
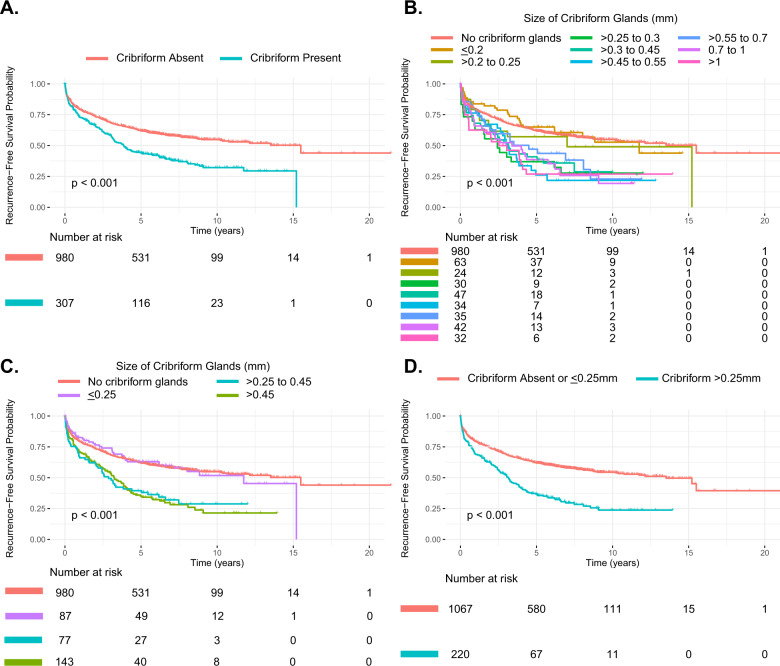
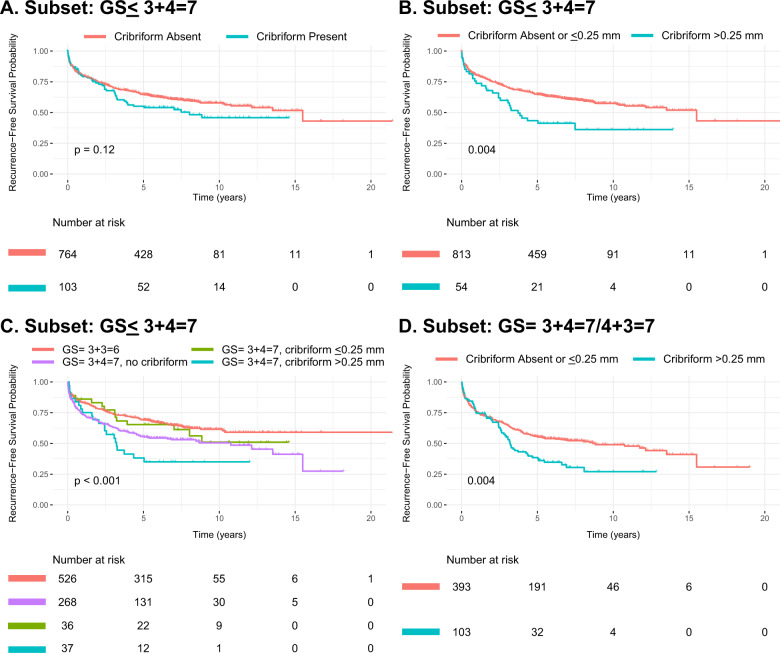
Cribriform growth pattern is well-established as an adverse pathologic feature in prostate cancer. The literature suggests "large" cribriform glands associate with aggressive behavior; however, published studies use varying definitions for "large". We aimed to identify an outcome-based quantitative cut-off for "large" vs "small" cribriform glands. We conducted an initial training phase using the tissue microarray based Canary retrospective radical prostatectomy cohort. Of 1287 patients analyzed, cribriform growth was observed in 307 (24%). Using Kaplan-Meier estimates of recurrence-free survival curves (RFS) that were stratified by cribriform gland size, we identified 0.25 mm as the optimal cutoff to identify more aggressive disease. In univariable and multivariable Cox proportional hazard analyses, size >0.25 mm was a significant predictor of worse RFS compared to patients with cribriform glands ≤0.25 mm, independent of pre-operative PSA, grade, stage and margin status (p < 0.001). In addition, two different subset analyses of low-intermediate risk cases (cases with Gleason score ≤ 3 + 4 = 7; and cases with Gleason score = 3 + 4 = 7/4 + 3 = 7) likewise demonstrated patients with largest cribriform diameter >0.25 mm had a significantly lower RFS relative to patients with cribriform glands ≤0.25 mm (each subset p = 0.004). Furthermore, there was no significant difference in outcomes between patients with cribriform glands ≤ 0.25 mm and patients without cribriform glands. The >0.25 mm cut-off was validated as statistically significant in a separate 419 patient, completely embedded whole-section radical prostatectomy cohort by biochemical recurrence, metastasis-free survival, and disease specific death, even when cases with admixed Gleason pattern 5 carcinoma were excluded. In summary, our findings support reporting cribriform gland size and identify 0.25 mm as an optimal outcome-based quantitative measure for defining "large" cribriform glands. Moreover, cribriform glands >0.25 mm are associated with potential for metastatic disease independent of Gleason pattern 5 adenocarcinoma.
筛状生长模式是前列腺癌中一种公认的不良病理特征。文献表明,“大”筛状腺体与侵袭性行为相关;然而,已发表的研究使用不同的定义来描述“大”筛状腺体。我们旨在确定基于结局的“大”与“小”筛状腺体的定量截断值。我们使用基于组织微阵列的 Canary 回顾性根治性前列腺切除术队列进行了初始的训练阶段。在分析的 1287 例患者中,有 307 例(24%)观察到筛状生长。使用按筛状腺体大小分层的无复发生存(RFS)的 Kaplan-Meier 估计曲线,我们发现 0.25mm 是识别侵袭性疾病的最佳截断值。在单变量和多变量 Cox 比例风险分析中,与筛状腺体≤0.25mm 的患者相比,大小>0.25mm 是 RFS 更差的显著预测因素,独立于术前 PSA、分级、分期和切缘状态(p<0.001)。此外,对低-中危病例(Gleason 评分≤3+4=7 例;Gleason 评分=3+4=7/4+3=7 例)的两个不同亚组分析同样表明,最大筛状直径>0.25mm 的患者的 RFS 明显低于筛状腺体≤0.25mm 的患者(每个亚组 p=0.004)。此外,筛状腺体≤0.25mm 的患者与无筛状腺体的患者之间的结局无显著差异。在另一个 419 例完全嵌入的整块前列腺切除术队列中,通过生化复发、无转移生存和疾病特异性死亡,0.25mm 的截断值被证明在统计学上是显著的,即使排除了混合的 Gleason 模式 5 癌病例。总之,我们的研究结果支持报告筛状腺体的大小,并确定 0.25mm 为定义“大”筛状腺体的最佳基于结局的定量测量。此外,大于 0.25mm 的筛状腺体与潜在的转移性疾病相关,而与 Gleason 模式 5 腺癌无关。