Robert J. Tomsich Institute of Pathology and Laboratory Medicine, Cleveland Clinic, Cleveland, OH, USA.
Department of Pathology and Laboratory Medicine, Emory University School of Medicine, Atlanta, GA, USA.
Histopathology. 2024 Oct;85(4):598-613. doi: 10.1111/his.15231. Epub 2024 Jun 3.
Histological grading of prostate cancer is a powerful prognostic tool, but current criteria for grade assignment are not fully optimised. Our goal was to develop and test a simplified histological grading model, based heavily on large cribriform/intraductal carcinoma, with optimised sensitivity for predicting metastatic potential.
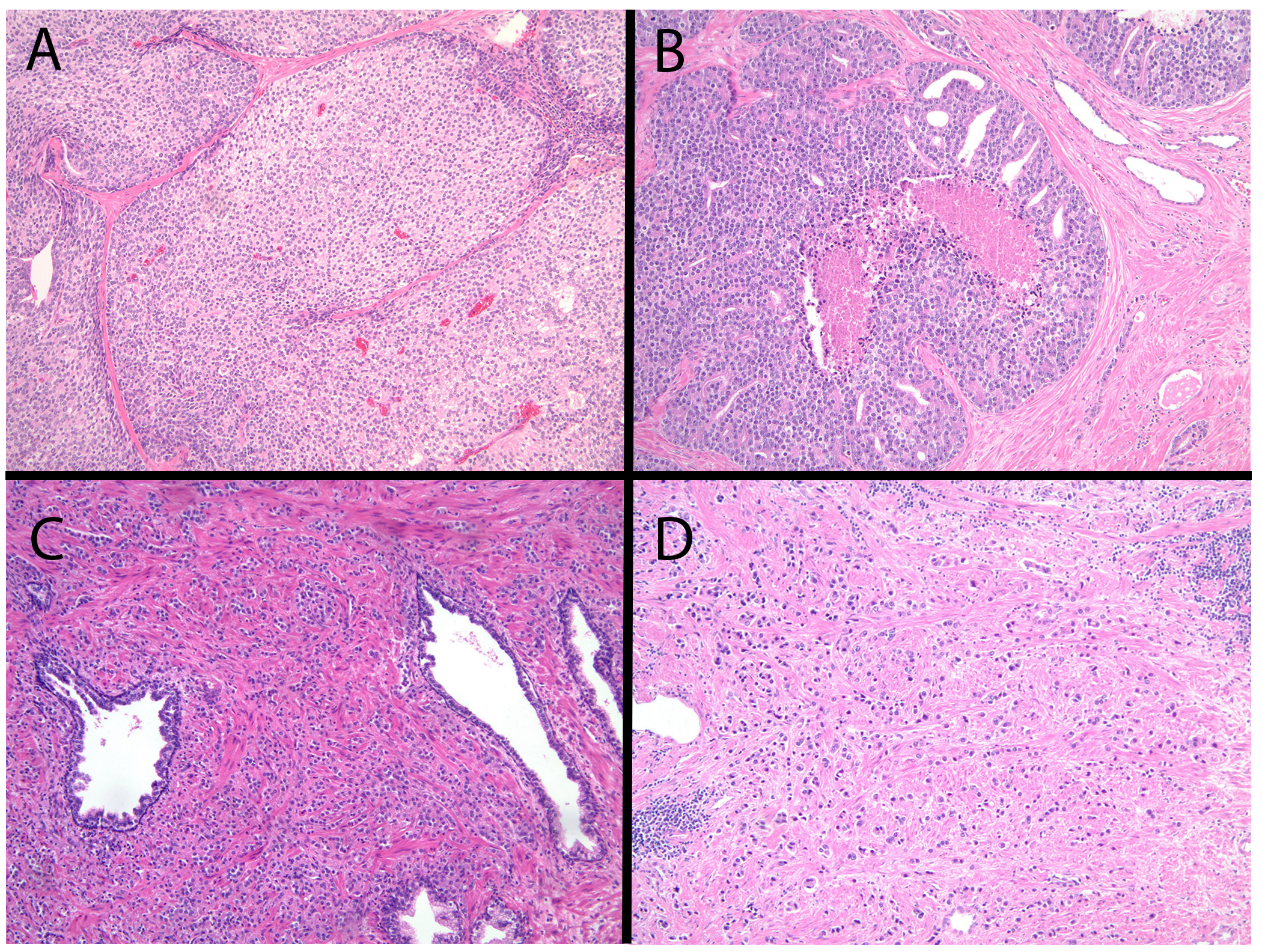
Two separate non-overlapping cohorts were identified: a 419-patient post-radical prostatectomy cohort with long term clinical follow-up and a 209-patient post-radical prostatectomy cohort in which all patients had pathologically confirmed metastatic disease. All prostatectomies were re-reviewed for high-risk histological patterns of carcinoma termed 'unfavourable histology'. Unfavourable histology is defined by any classic Gleason pattern 5 component, any large cribriform morphology (> 0.25 mm) or intraductal carcinoma, complex intraluminal papillary architecture, grade 3 stromogenic carcinoma and complex anastomosing cord-like growth. For the outcome cohort, Kaplan-Meier analysis compared biochemical recurrence, metastasis and death between subjects with favourable and unfavourable histology, stratified by pathological stage and grade group. Multivariable Cox proportional hazards models evaluated adding unfavourable histology to the Memorial Sloan Kettering Cancer Center (MSKCC) post-prostatectomy nomogram and stratification by percentage of unfavourable histology. At 15 years unfavourable histology predicted biochemical recurrence, with sensitivity of 93% and specificity of 88%, metastatic disease at 100 and 48% and death at 100 and 46%. Grade group 2 prostate cancers with unfavourable histology were associated with metastasis independent of pathological stage, while those without had no risk. Histological models for prediction of metastasis based on only large cribriform/intraductal carcinoma or increasing diameter of cribriform size improved specificity, but with lower sensitivity. Multivariable Cox proportional hazards models demonstrated that unfavourable histology significantly improved discriminatory power of the MSKCC post-prostatectomy nomogram for biochemical failure (likelihood ratio test P < 0.001). In the retrospective review of a separate RP cohort in which all patients had confirmed metastatic disease, none had unequivocal favourable histology.
Unfavourable histology at radical prostatectomy is associated with metastatic risk, predicted adverse outcomes better than current grading and staging systems and improved the MSKCC post-prostatectomy nomogram. Most importantly, unfavourable histology stratified grade group 2 prostate cancers into those with and without metastatic potential, independent of stage. While unfavourable histology is driven predominantly by large cribriform/intraductal carcinoma, the recognition and inclusion of other specific architectural patterns add to the sensitivity for predicting metastatic disease. Moreover, a simplified dichotomous model improves communication and could increase implementation.
前列腺癌的组织学分级是一种强大的预后工具,但目前用于分级的标准并非完全优化。我们的目标是开发和测试一种简化的组织学分级模型,该模型主要基于大筛状/管内癌,具有优化的预测转移潜能的敏感性。
确定了两个独立的不重叠队列:一个是 419 例根治性前列腺切除术患者队列,具有长期临床随访,另一个是 209 例根治性前列腺切除术患者队列,所有患者均经病理证实存在转移性疾病。所有前列腺切除术均重新审查高危组织学模式的癌,称为“不良组织学”。不良组织学定义为任何经典的 Gleason 模式 5 成分、任何大筛状形态(>0.25mm)或管内癌、复杂腔内乳头状结构、3 级基质性癌和复杂吻合索状生长。对于结局队列,Kaplan-Meier 分析比较了有利组织学和不利组织学患者的生化复发、转移和死亡情况,按病理分期和分级组分层。多变量 Cox 比例风险模型评估了将不良组织学添加到 Memorial Sloan Kettering Cancer Center(MSKCC)前列腺切除术后nomogram 中,并按不良组织学百分比进行分层。在 15 年时,不良组织学预测生化复发,敏感性为 93%,特异性为 88%,预测转移的敏感性为 100%和 48%,死亡的敏感性为 100%和 46%。有不良组织学的 2 级前列腺癌与转移相关,独立于病理分期,而没有不良组织学的则没有风险。仅基于大筛状/管内癌或增加筛状大小的转移预测模型提高了特异性,但敏感性较低。多变量 Cox 比例风险模型表明,不良组织学显著提高了 MSKCC 前列腺切除术后 nomogram 对生化失败的判别能力(似然比检验 P<0.001)。在对另一例根治性前列腺切除术患者队列的回顾性分析中,所有患者均经病理证实存在转移性疾病,无一例具有明确的有利组织学。
根治性前列腺切除术后的不良组织学与转移风险相关,预测不良预后优于目前的分级和分期系统,并改善了 MSKCC 前列腺切除术后 nomogram。最重要的是,不良组织学将 2 级前列腺癌分为有和无转移潜能的患者,独立于分期。虽然不良组织学主要由大筛状/管内癌驱动,但识别和纳入其他特定的结构模式可提高预测转移疾病的敏感性。此外,简化的二项式模型可改善沟通并提高实施率。