Beijing Emergency Medical Center, Beijing, 100031, China.
BMC Emerg Med. 2022 Feb 11;22(1):25. doi: 10.1186/s12873-022-00581-0.
To investigate and understand the determinants of decisions not to attempt resuscitation following out-of-hospital cardiac arrest, to contribute to establishing rules that are appropriate to China.
We recruited participants through directors of emergency medical services across China. A 28-question web survey was available between February 5 and March 6, 2021 that targeted demographic information and views on emergency work and cardiopulmonary resuscitation. Each question was assigned a value between 1 and 7 based on the level of importance from low to high. T-tests, one-way analysis of variance, and Kruskal-Wallis H-tests were used to compare continuous variables. Binary logistic regression analysis was used to identify factors influencing when people considered it suitable to initiate cardiopulmonary resuscitation.
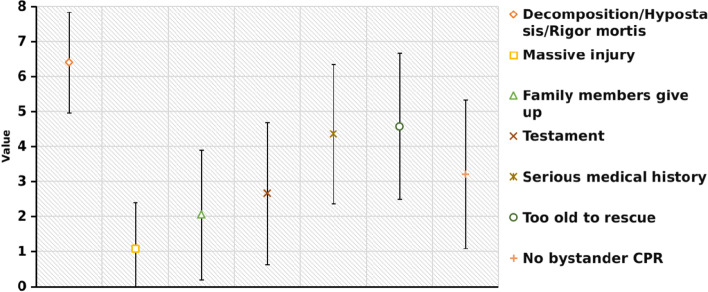
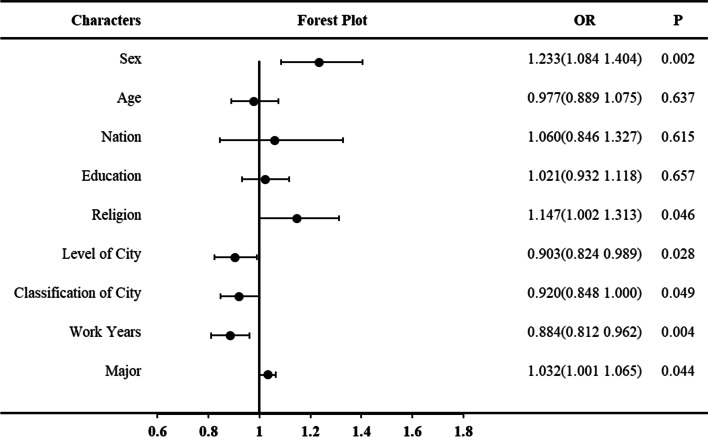
The study involved 4289 participants from 31 provinces, autonomous regions and municipalities in mainland China, of whom 52.8% were male. The top three reasons for not attempting cardiopulmonary resuscitation were decomposition/hypostasis/rigor mortis (6.39 ± 1.44 points), massive injury (4.57 ± 2.08 points) and family members' preference (4.35 ± 1.98 points). In total, 2761 (64.4%) thought emergency services should not attempt cardiopulmonary resuscitation when cardiac arrest had happened more than 30 min before, and there had been no bystander cardiopulmonary resuscitation. Gender (OR 1.233, p = 0.002), religion (OR 1.147, p = 0.046), level (OR 0.903, p = 0.028) or classification of city (OR 0.920, p = 0.049), years of work experience (OR 0.884, p = 0.004), and major (OR 1.032, p = 0.044) all influenced how long after cardiac arrest was considered suitable for initiating cardiopulmonary resuscitation.
Chinese emergency physicians have different perceptions of when not to attempt resuscitation to those practicing elsewhere. The existing guidelines for resuscitation are not suitable for China, and China-specific guidelines need to be established.
调查和了解院外心脏骤停后不尝试复苏的决定因素,有助于制定适合中国的规则。
我们通过中国各地的急救医疗服务主任招募参与者。2021 年 2 月 5 日至 3 月 6 日期间,可通过 28 个问题的网络调查获得目标人群的人口统计学信息和对急救工作及心肺复苏术的看法。根据重要性从低到高,为每个问题分配 1 到 7 之间的值。使用 t 检验、单因素方差分析和 Kruskal-Wallis H 检验比较连续变量。使用二元逻辑回归分析确定影响人们认为何时适合开始心肺复苏的因素。
本研究涉及中国大陆 31 个省、自治区和直辖市的 4289 名参与者,其中 52.8%为男性。不尝试心肺复苏的前三个原因是尸僵/尸斑/僵硬(6.39±1.44 分)、严重损伤(4.57±2.08 分)和家属的偏好(4.35±1.98 分)。总共 2761 人(64.4%)认为如果在心脏骤停发生 30 分钟以上且没有旁观者心肺复苏术的情况下,急救服务不应该尝试心肺复苏。性别(OR 1.233,p=0.002)、宗教(OR 1.147,p=0.046)、级别(OR 0.903,p=0.028)或城市分类(OR 0.920,p=0.049)、工作年限(OR 0.884,p=0.004)和专业(OR 1.032,p=0.044)均影响人们认为心脏骤停后多久开始心肺复苏术是合适的。
中国急救医生对不尝试复苏的看法与其他地方的医生不同。现有的复苏指南不适合中国,需要制定适合中国的指南。