Sanborn Ryan M, Badger Gary J, Yen Yi-Meng, Murray Martha M, Christino Melissa A, Proffen Benedikt, Sant Nicholas, Barnett Samuel, Fleming Braden C, Kramer Dennis E, Micheli Lyle J
Division of Sports Medicine, Department of Orthopaedic Surgery, Boston Children's Hospital, Boston, Massachusetts, USA.
Department of Medical Biostatistics, University of Vermont, Burlington, Vermont, USA.
Orthop J Sports Med. 2022 Feb 9;10(2):23259671211070542. doi: 10.1177/23259671211070542. eCollection 2022 Feb.
Previous clinical studies have shown that psychological factors have significant effects on an athlete's readiness to return to sport after anterior cruciate ligament (ACL) reconstruction (ACLR).
We hypothesized that patients who underwent bridge-enhanced ACL restoration (BEAR) would have higher levels of psychological readiness to return to sport compared with patients who underwent ACLR.
Randomized controlled trial; Level of evidence, 1.
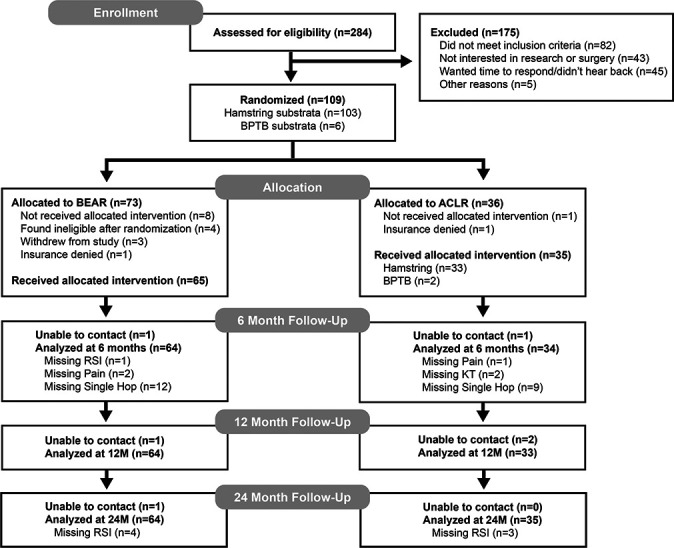
A total of 100 patients (median age, 17 years; median preoperative Marx activity score, 16) with complete midsubstance ACL injuries were randomized to either the BEAR procedure (n = 65) or autograft ACLR (n = 35 [33 hamstring and 2 bone--patellar tendon-bone]) and underwent surgery within 45 days of injury. Objective, functional, and patient-reported outcomes, including the ACL--Return to Sport after Injury (ACL-RSI) scale, were assessed at 6, 12, and 24 months postoperatively.
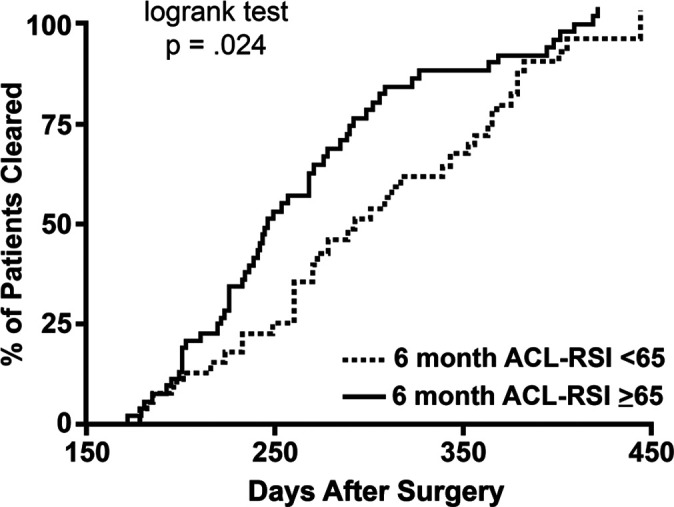
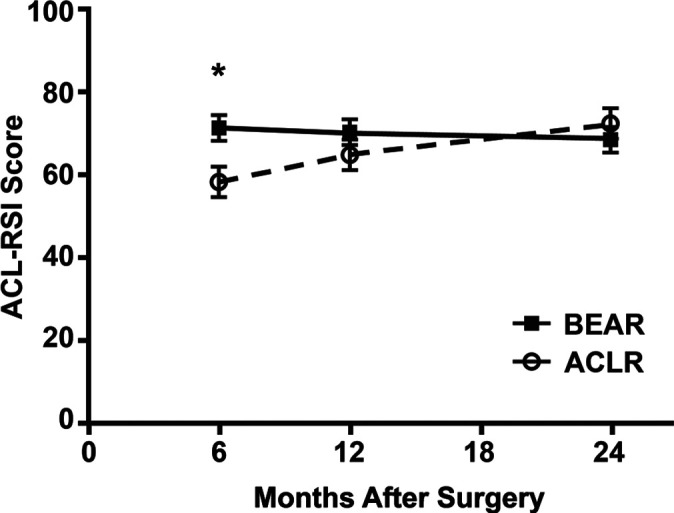
Patients who underwent the BEAR procedure had significantly higher ACL-RSI scores at 6 months compared with those who underwent ACLR (71.1 vs 58.2; = .008); scores were similar at 12 and 24 months. Baseline factors independently predictive of higher ACL-RSI scores at 6 months were having a BEAR procedure and participating in level 1 sports prior to injury, explaining 15% of the variability in the scores. Regression analysis of baseline and 6-month outcomes as predictors indicated that the International Knee Documentation Committee (IKDC) score at 6 months explained 45% of the 6-month ACL-RSI variance. Subsequent analysis with IKDC excluded from the model indicated that decreased pain, increased hamstring and quadriceps strength in the surgical limb, and decreased side-to-side difference in anteroposterior knee laxity were significant predictors of a higher ACL-RSI score at 6 months, explaining 34% of the variability in scores. Higher ACL-RSI score at 6 months was associated with earlier clearance to return to sports.
Patients who underwent the BEAR procedure had higher ACL-RSI scores at 6 months postoperatively. Better ACL-RSI scores at 6 months were related most strongly to higher IKDC scores at 6 months and were also associated with lower pain levels, better muscle recovery, and less knee laxity at 6 months.
NCT02664545 (ClinicalTrials.gov identifier).
先前的临床研究表明,心理因素对前交叉韧带(ACL)重建(ACLR)后运动员恢复运动的准备情况有显著影响。
我们假设,与接受ACLR的患者相比,接受桥接增强ACL修复(BEAR)的患者恢复运动的心理准备水平更高。
随机对照试验;证据等级,1级。
共有100例完全性ACL中部损伤患者(中位年龄17岁;术前马克思活动评分中位数16)被随机分为BEAR手术组(n = 65)或自体移植ACLR组(n = 35 [33例腘绳肌和2例骨-髌腱-骨]),并在受伤后45天内接受手术。在术后6、12和24个月评估客观、功能和患者报告的结果,包括ACL损伤后恢复运动(ACL-RSI)量表。
与接受ACLR的患者相比,接受BEAR手术的患者在术后6个月时的ACL-RSI评分显著更高(71.1对58.2;P = 0.008);在12个月和24个月时评分相似。独立预测术后6个月较高ACL-RSI评分的基线因素是接受BEAR手术和受伤前参加1级运动,这解释了评分变异性的15%。将基线和6个月结果作为预测因素的回归分析表明,6个月时的国际膝关节文献委员会(IKDC)评分解释了6个月时ACL-RSI方差的45%。随后在模型中排除IKDC的分析表明,疼痛减轻、手术侧腘绳肌和股四头肌力量增加以及膝关节前后向松弛度的左右差异减小是术后6个月较高ACL-RSI评分的显著预测因素,解释了评分变异性的34%。术后6个月较高的ACL-RSI评分与更早获准恢复运动相关。
接受BEAR手术的患者在术后6个月时的ACL-RSI评分更高。术后6个月更好的ACL-RSI评分与6个月时更高的IKDC评分最密切相关,也与6个月时更低的疼痛水平、更好的肌肉恢复和更小的膝关节松弛度相关。
NCT02664545(ClinicalTrials.gov标识符)