Chlabicz Małgorzata, Jamiołkowski Jacek, Łaguna Wojciech, Dubatówka Marlena, Sowa Paweł, Łapińska Magda, Szpakowicz Anna, Zieleniewska Natalia, Zalewska Magdalena, Raczkowski Andrzej, Kamiński Karol A
Department of Population Medicine and Lifestyle Diseases Prevention, Medical University of Białystok, 15-259 Białystok, Poland.
Department of Invasive Cardiology, Medical University of Białystok, 15-259 Białystok, Poland.
J Clin Med. 2022 Jan 28;11(3):688. doi: 10.3390/jcm11030688.
Cardiovascular diseases (CVD) are still the leading cause of death in developed countries. The aim of this study was to calculate the potential for CV risk reduction when using three different prevention strategies to evaluate the effect of primary prevention.
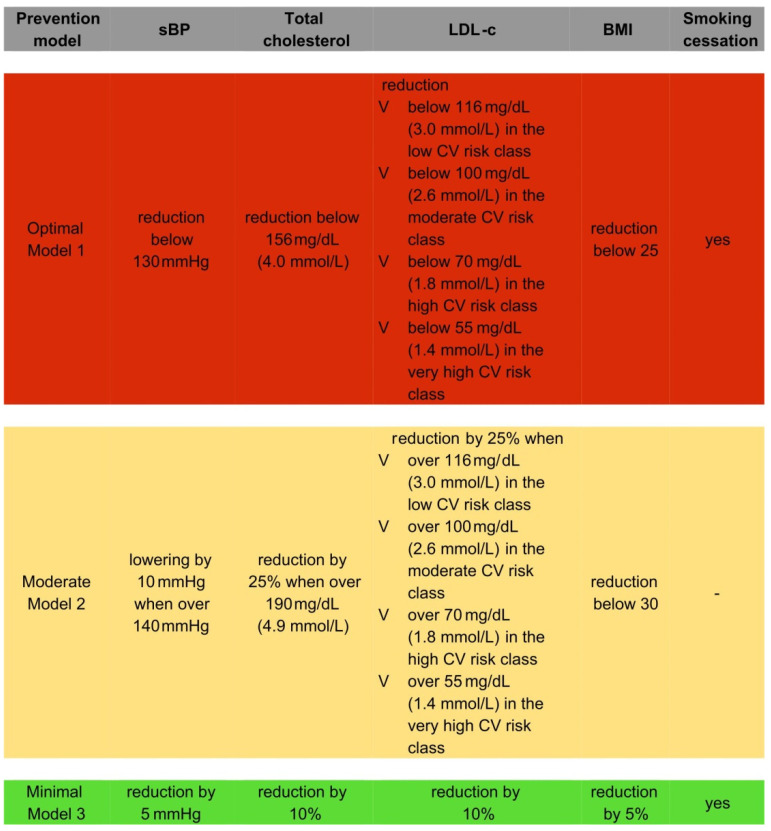
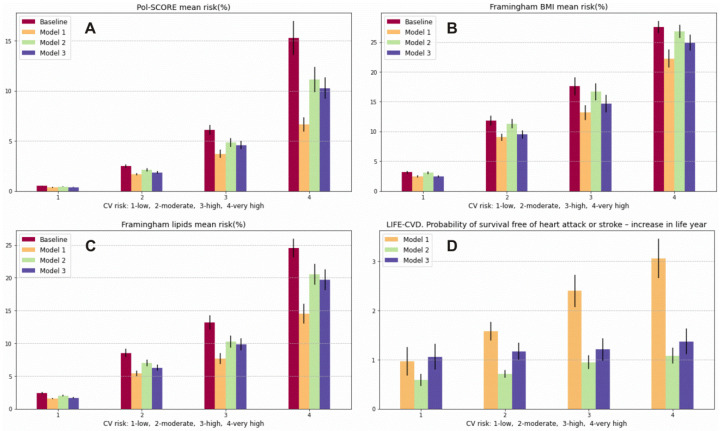
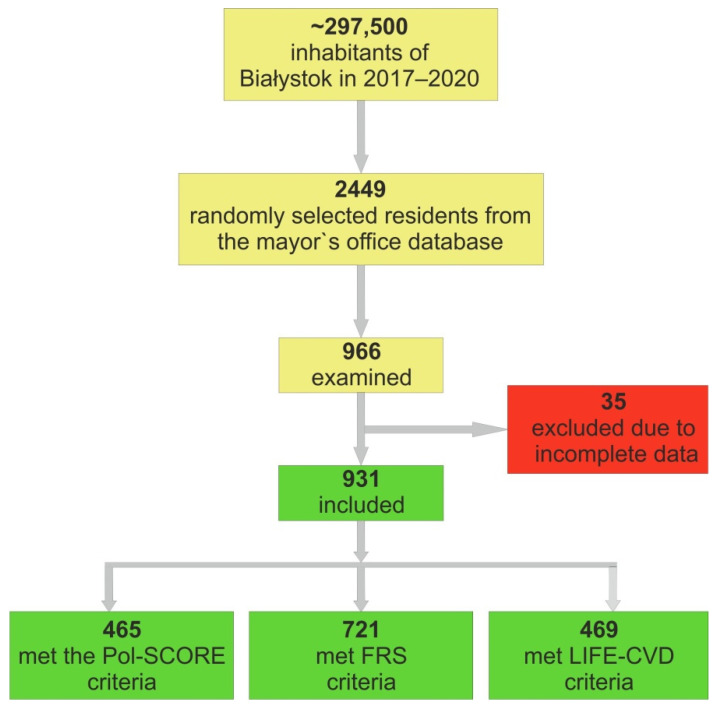
A total of 931 individuals aged 20-79 years old from the Bialystok PLUS Study were analyzed. The study population was divided into CV risk classes. The Systematic Coronary Risk Estimation (SCORE), Framingham Risk Score (FRS), and LIFE-CVD were used to assess CV risk. The optimal prevention strategy assumed the attainment of therapeutic goals according to the European guidelines. The moderate strategy assumed therapeutic goals in participants with increased risk factors: a reduction in systolic blood pressure by 10 mmHg when it was above 140 mmHg, a reduction in total cholesterol by 25% when it was above 190 mg/dL, and a reduction in body mass index below 30. The minimal prevention strategy assumed that CV risk would be lowered by lifestyle modifications. The greatest CV risk reduction was achieved in the optimal model and then in the minimal model, and the lowest risk reduction was achieved in the moderate model, e.g., using the optimal model of prevention (Model 1). In the total population, we achieved a reduction of -1.74% in the 10-year risk of CVD death (SCORE) in relation to the baseline model, a -0.85% reduction when using the moderate prevention model (Model 2), and a -1.11% reduction when using the minimal prevention model (Model 3). However, in the low CV risk class, the best model was the minimal one (risk reduction of -0.72%), which showed even better results than the optimal one (reduction of -0.69%) using the FRS.
A strategy based on lifestyle modifications in a population without established CVD could be more effective than the moderate strategy used in the present study. Moreover, applying a minimal strategy to the low CV risk class population may even be beneficial for an optimal model.
心血管疾病(CVD)仍是发达国家的主要死因。本研究的目的是计算使用三种不同预防策略评估一级预防效果时降低心血管风险的潜力。
对来自比亚韦斯托克PLUS研究的931名年龄在20 - 79岁的个体进行了分析。研究人群被分为心血管风险类别。使用系统性冠状动脉风险评估(SCORE)、弗雷明汉风险评分(FRS)和LIFE - CVD来评估心血管风险。最佳预防策略假定根据欧洲指南实现治疗目标。适度策略假定在具有增加的风险因素的参与者中实现治疗目标:收缩压高于140 mmHg时降低10 mmHg,总胆固醇高于190 mg/dL时降低25%,体重指数降至30以下。最小预防策略假定通过生活方式改变降低心血管风险。在最佳模型中实现了最大的心血管风险降低,其次是最小模型,而在适度模型中实现的风险降低最低,例如使用最佳预防模型(模型1)。在总体人群中,与基线模型相比,我们使用最佳预防模型(模型1)使心血管疾病死亡的10年风险降低了 - 1.74%(SCORE),使用适度预防模型(模型2)降低了 - 0.85%,使用最小预防模型(模型3)降低了 - 1.11%。然而,在低心血管风险类别中,最佳模型是最小模型(风险降低 - 0.72%),使用FRS时其结果甚至优于最佳模型(降低 - 0.69%)。
在没有已确诊心血管疾病的人群中,基于生活方式改变的策略可能比本研究中使用的适度策略更有效。此外,对低心血管风险类别的人群应用最小策略甚至可能对最佳模型有益。