Department of Vascular Medicine, University Medical Center Utrecht, Heidelberglaan 100, 3584 CX Utrecht, Netherlands.
Johns Hopkins Ciccarone Center for the Prevention of Heart Disease, Johns Hopkins Hospital, 1800 Orleans St, Baltimore, MD 21287, USA.
Eur Heart J. 2020 Mar 14;41(11):1190-1199. doi: 10.1093/eurheartj/ehz239.
The benefit an individual can expect from preventive therapy varies based on risk-factor burden, competing risks, and treatment duration. We developed and validated the LIFEtime-perspective CardioVascular Disease (LIFE-CVD) model for the estimation of individual-level 10 years and lifetime treatment-effects of cholesterol lowering, blood pressure lowering, antithrombotic therapy, and smoking cessation in apparently healthy people.
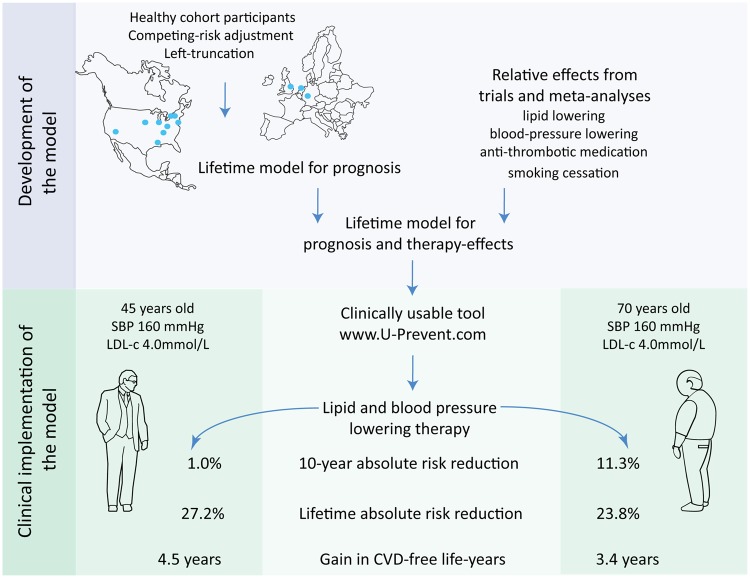
Model development was conducted in the Multi-Ethnic Study of Atherosclerosis (n = 6715) using clinical predictors. The model consists of two complementary Fine and Gray competing-risk adjusted left-truncated subdistribution hazard functions: one for hard cardiovascular disease (CVD)-events, and one for non-CVD mortality. Therapy-effects were estimated by combining the functions with hazard ratios from preventive therapy trials. External validation was performed in the Atherosclerosis Risk in Communities (n = 9250), Heinz Nixdorf Recall (n = 4177), and the European Prospective Investigation into Cancer and Nutrition-Netherlands (n = 25 833), and Norfolk (n = 23 548) studies. Calibration of the LIFE-CVD model was good and c-statistics were 0.67-0.76. The output enables the comparison of short-term vs. long-term therapy-benefit. In two people aged 45 and 70 with otherwise identical risk-factors, the older patient has a greater 10-year absolute risk reduction (11.3% vs. 1.0%) but a smaller gain in life-years free of CVD (3.4 vs. 4.5 years) from the same therapy. The model was developed into an interactive online calculator available via www.U-Prevent.com.
The model can accurately estimate individual-level prognosis and treatment-effects in terms of improved 10-year risk, lifetime risk, and life-expectancy free of CVD. The model is easily accessible and can be used to facilitate personalized-medicine and doctor-patient communication.
个人从预防治疗中获得的益处取决于风险因素负担、竞争风险和治疗持续时间。我们开发并验证了终生视角心血管疾病(LIFE-CVD)模型,用于估计胆固醇降低、血压降低、抗血栓治疗和戒烟在貌似健康人群中的个体 10 年和终生治疗效果。
使用临床预测因素在多民族动脉粥样硬化研究(n=6715)中进行模型开发。该模型由两个互补的 Fine 和 Gray 竞争风险调整的左截断亚分布风险函数组成:一个用于硬心血管疾病(CVD)事件,另一个用于非 CVD 死亡率。通过将函数与预防性治疗试验的风险比相结合来估计治疗效果。在动脉粥样硬化风险社区研究(n=9250)、Heinz Nixdorf 召回研究(n=4177)、欧洲癌症前瞻性调查-荷兰研究(n=25833)和诺福克研究(n=23548)中进行了外部验证。LIFE-CVD 模型的校准良好,C 统计量为 0.67-0.76。该模型的输出可用于比较短期和长期治疗效益。在两名年龄分别为 45 岁和 70 岁、其他风险因素相同的患者中,年龄较大的患者在 10 年内的绝对风险降低(11.3%对 1.0%)更大,但从相同治疗中获得的无 CVD 生存年限(3.4 年对 4.5 年)增长较小。该模型被开发成一个交互式在线计算器,可通过 www.U-Prevent.com 获得。
该模型可以准确估计个体水平的预后和治疗效果,包括改善 10 年风险、终生风险和无 CVD 的预期寿命。该模型易于访问,可以用于促进个性化医疗和医患沟通。